



Eosinophilia is defined as a peripheral blood eosinophil count > 500/mcL (> 0.5 × 109/L). Causes and associated disorders are myriad but often represent an allergic reaction, including reactions to medications or a parasitic infection. Eosinophilia can be reactive (secondary) or the primary manifestation of a hematologic disorder. Diagnosis involves selective testing directed at clinically suspected causes. Treatment of primary clonal eosinophilia includes glucocorticoids and, depending upon specific genetic abnormalities, tyrosine kinase inhibitors and/or monoclonal antibodies. Treatment is directed at the other underlying causes in secondary eosinophilia.
Eosinophilia has features of an immune response: an agent such as Trichinella spiralis invokes a primary response with relatively low levels of eosinophils, whereas repeated exposures result in an augmented or secondary eosinophilic response. Several compounds released by mast cells and basophils induce IgE-mediated eosinophil production. Such substances include eosinophil chemotactic factor of anaphylaxis, leukotriene B4, complement complex (C5-C6-C7), and histamine (over a narrow range of concentration).
Peripheral eosinophilia is characterized as:
Mild: 500 to 1500/mcL (0.5 to 1.5 × 109/L)
Moderate: 1500 to 5000/mcL (1.5 to 5 × 109/L)
Severe: > 5000/mcL (> 5 × 109/L)
Mild eosinophilia itself does not cause symptoms, but levels ≥ 1500/mcL (≥ 1.5 × 109/L) may cause organ damage if they persist. Organ damage typically occurs because of tissue inflammation and reaction to the cytokines and chemokines released by the eosinophils as well as to immune cells that are recruited to the tissues. Although any organ may be involved, the heart, lungs, spleen, skin, and nervous system are typically affected (for manifestations, see table ).
Occasionally, patients with very severe eosinophilia (eg, eosinophil counts of > 100,000/mcL [> 100 × 109/L]), usually with eosinophilic leukemia, develop complications when eosinophils form aggregates that occlude small blood vessels, causing tissue ischemia and microinfarctions. Manifestations typically include those of brain or lung hypoxia (eg, encephalopathy, dyspnea, respiratory failure).

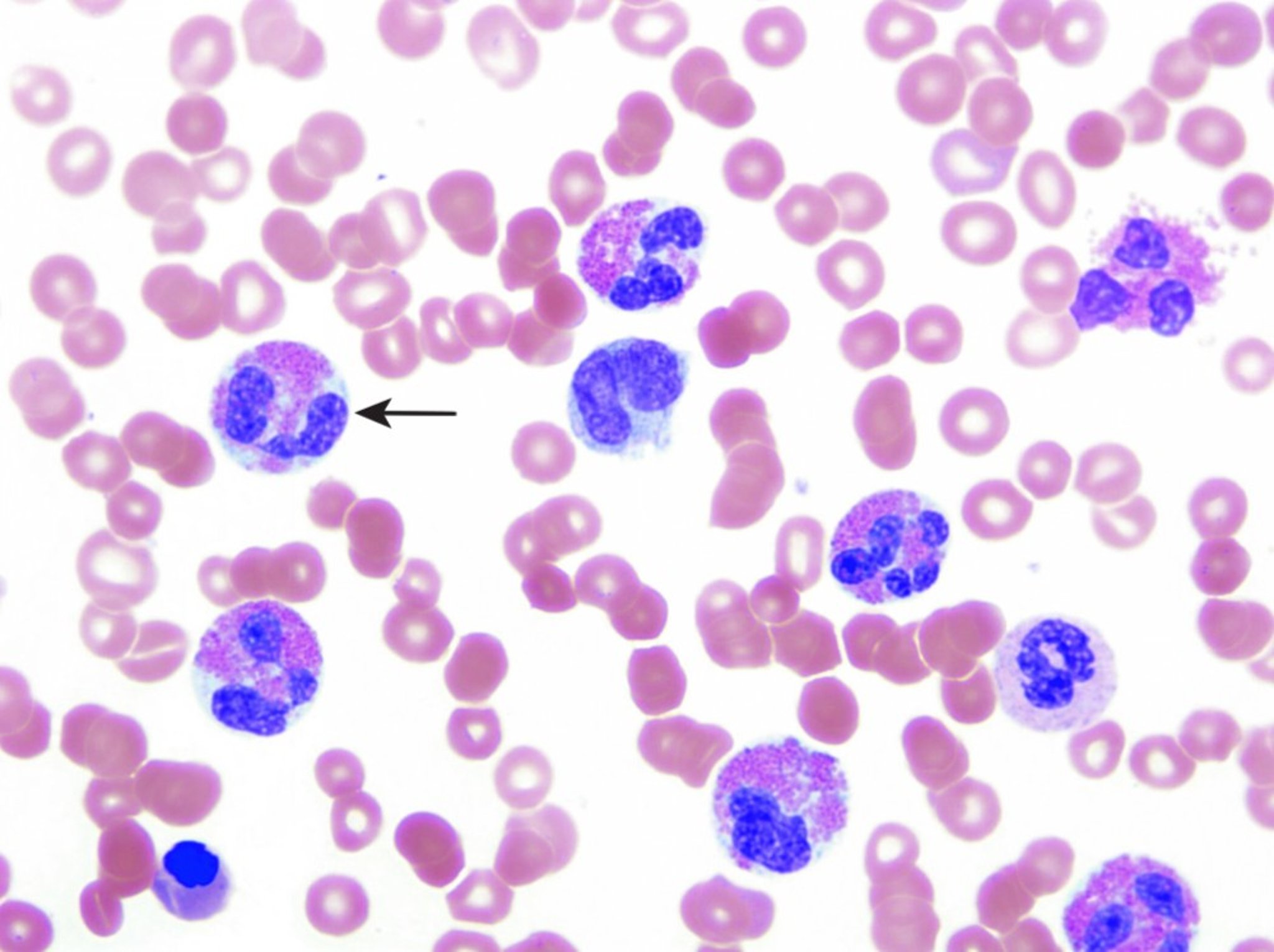
This image shows eosinophilic cells (arrow).
© Springer Science+Business Media
Idiopathic hypereosinophilic syndrome is a condition characterized by peripheral blood eosinophilia with manifestations of organ system involvement or dysfunction directly related to eosinophilia in patients who do not have a parasitic or allergic disorder, a clonal disorder of hematopoiesis, or another cause of eosinophilia.

Etiology of Eosinophilia
Eosinophilia may be:
Primary: A clonal proliferation of eosinophils associated with hematologic disorders such as leukemias and myeloproliferative neoplasms
Secondary: Caused by or associated with nonhematologic disorders (see table )
Idiopathic: Cause cannot be identified
The most common cause of eosinophilia in the United States is:
Allergic or atopic disorders (typically respiratory or dermatologic)
In cases caused by allergic or atopic disorders, eosinophilia is often mild to moderate (1).
Other common causes of eosinophilia include:
Medication reactions (both allergic and non-allergic)
Infections (typically parasitic)
Certain tumors (hematologic or solid, benign or malignant)
Patients with eosinophilic medication reactions may be asymptomatic or have various syndromes, including interstitial nephritis, serum sickness, cholestatic jaundice, hypersensitivity vasculitis, and immunoblastic lymphadenopathy. Severe cutaneous reactions have been reported with use of immune checkpoint inhibitors in patients with cancer (2).
Eosinophilia-myalgia syndrome (EMS) is a rare multisystemic disorder characterized by severe myalgias and peripheral eosinophilia; the cause is unknown. However, in 1989, several hundred patients were reported to have developed this syndrome after taking L-tryptophan for sedation or psychotropic support (3). This syndrome was probably caused by a contaminant rather than by L-tryptophan. The symptoms, including severe muscle pain, tenosynovitis, muscle edema, and rash, lasted weeks to months, and several deaths occurred. Thus far, no cases of eosinophilia myalgia syndrome have been definitely linked to 5-hydroxytryptophan dietary supplements (4).
Drug reaction with eosinophilia and systemic symptoms (DRESS) is a rare syndrome characterized by fever, morbilliform rash, facial edema, eosinophilia, atypical lymphocytosis, lymphadenopathy, and signs and symptoms related to end-organ involvement (typically, heart, lungs, spleen, skin, nervous system) (5, 6). It requires urgent evaluation and treatment to prevent severe complications and death. Different medications have varying propensity to cause DRESS. The most common causes are allopurinol, vancomycin, lamotrigine, carbamazepine, and sulfamethoxazole/trimethoprim. Aromatic antiseizure medications (eg, carbamazepine, lamotrigine) confer the highest risk, followed by allopurinol and sulfonamide antibiotics (7, 8).
Almost any parasitic invasion of tissues can elicit eosinophilia, but protozoa (amoeba) and noninvasive metazoa usually do not.
Of hematologic tumors, Hodgkin lymphoma may elicit marked eosinophilia, whereas eosinophilia is less common in non-Hodgkin lymphoma, chronic myeloid leukemia, and acute lymphoblastic leukemia.
The pulmonary infiltrates that may occur with peripheral eosinophilia are part of a spectrum of clinical disorders, which can be infectious (eg, parasitic or fungal), autoimmune (eg, eosinophilic granulomatosis with polyangiitis) or inflammatory (eg, toxin or malignancy) in nature.
Eosinophilic esophagitis is an increasingly recognized condition characterized by vomiting and dysphagia. To make a diagnosis, esophageal biopsy should show at least 15 eosinophils per high power field. Treatment includes proton pump inhibitors, budesonide, food elimination trials, and sometimes esophageal dilation (9). Dupilumab may also have therapeutic benefit (10).
Important Disorders and Treatments Associated With Eosinophilia
Cause or Associated Disorder | Examples |
|---|---|
Allergic or atopic disorders | Allergic bronchopulmonary aspergillosis Episodic angioedema with eosinophilia Medication reactions (eg, to antibiotics or NSAIDs) Milk-protein allergy Occupational lung disease |
Systemic rheumatic diseases, vasculitic or granulomatous disorders (especially those involving the lungs) | Eosinophilic granulomatosis with polyangiitis Idiopathic eosinophilic synovitis Kimura disease Post myocardial infarction syndrome (Dressler syndrome) Progressive systemic sclerosis (scleroderma) |
Endocrine disorders | Adrenal hypofunction |
Immune disorders (often with eczema) | Congenital immunodeficiency syndrome (eg, IgA deficiency, hyper-IgE syndrome, Wiskott-Aldrich syndrome) |
Acute leukemias and myeloproliferative neoplasms | Acute or chronic eosinophilic leukemia Acute lymphoblastic leukemia, particularly B-cell acute lymphoblastic leukemia (B-ALL) with t(5;14)(q31;q32) - IGH–IL3 rearrangement* |
Nonparasitic infections | Chlamydial pneumonia of infancy Coccidioidomycosis (acute) Infectious lymphocytosis Mycobacterial disease |
Parasitic infections (especially due to tissue-invasive metazoans) | Cysticercosis (caused by Taenia solium) Pneumocystis jirovecii infection |
Skin disorders | |
Syndromes of pulmonary infiltration with eosinophilia | Allergic bronchopulmonary aspergillosis Chronic eosinophilic pneumonia Eosinophilic granulomatosis with polyangiitis (Churg-Strauss syndrome) Tropical pulmonary eosinophilia |
Non-myeloproliferative cancers | Angioimmunoblastic T-cell lymphoma (previously known as angioimmunoblastic lymphadenopathy with dysproteinemia or AILD) in association with systemic symptoms and autoimmune hemolytic anemia Carcinomas and sarcomas of the lung, pancreas, colon, cervix, or ovary |
Miscellaneous | Familial eosinophilia Peritoneal dialysis Radiation therapy |
* Fournier B, Balducci E, Duployez N, et al. B-ALL With t(5;14)(q31;q32); IGH-IL3 Rearrangement and Eosinophilia: A Comprehensive Analysis of a Peculiar IGH-Rearranged B-ALL. Front Oncol. 2019;9:1374. doi:10.3389/fonc.2019.01374 | |
NSAID = nonsteroidal anti-inflammatory drug. | |
Evaluation of Eosinophilia
Numerous conditions can cause eosinophilia. Common causes include allergic, infectious, and neoplastic disorders.
History
The questions most likely to be helpful pertain to the following:
Travel (suggesting possible parasite exposure)
Allergies
Autoimmune disorders
Medication use
Use of herbal products and dietary supplements
Systemic symptoms (eg, fever, weight loss, myalgias, arthralgias, rashes, lymphadenopathy)
New dietary exposures
Systemic symptoms suggest that a detailed evaluation for an infectious, neoplastic, systemic rheumatic disease, or other systemic disorder should be done. Other important parts of the history include family history of blood disorders and a complete review of systems, including symptoms of allergies and pulmonary, cardiac, gastrointestinal (GI), and neurologic dysfunction.
Physical examination
A general physical examination should focus on the heart, skin, and neurologic and pulmonary systems. Certain physical findings may suggest causes or associated disorders. Examples include rash (allergic, dermatologic, or vasculitic disorders), abnormal lung findings (asthma, lung infections, or syndromes of pulmonary infiltration with eosinophilia), and generalized lymphadenopathy or splenomegaly (myeloproliferative neoplasms or cancer).
Testing
Eosinophilia is typically recognized when a complete blood count (CBC) is done for other reasons. Additional testing often includes the following (1,2):
Stool ova and parasite testing
Other tests to detect organ damage or for specific causes based on clinical findings
In general, if a medication or allergic cause is not suspected based on clinical findings, 3 stool specimens should be examined for ova and parasites; however, negative findings do not exclude a parasitic cause (eg, trichinosis requires a muscle biopsy; toxocariasis and filarial infections require other tissue biopsies; duodenal aspirates may be needed to exclude specific parasites, such as Strongyloides).
Other specific diagnostic tests are determined by the clinical findings (particularly travel history) and may include chest radiograph, urinalysis, liver and kidney tests, and serologic tests for parasitic and systemic rheumatic diseases. If patients have generalized lymphadenopathy, splenomegaly, or systemic symptoms, blood tests are done. An elevated serum vitamin B12 level or abnormalities on the peripheral blood smear suggest an underlying myeloproliferative neoplasm, and a bone marrow aspirate and biopsy with cytogenetic studies may be helpful.
If a routine evaluation does not reveal a cause, tests are done to detect organ damage. Testing can include some of the tests previously mentioned as well as lactate dehydrogenase (LDH) and liver tests (suggesting liver damage or possibly a myeloproliferative neoplasm). Echocardiography, serum troponin levels, and pulmonary function tests are performed in patients with cardiopulmonary manifestations. In those with suspected vasculitis or asthma, an anti-neutrophil cytoplasmic antibody (ANCA) can be measured, and if the titer is elevated, high-resolution CT is recommended.
Evaluation references
1. Klion AD. Approach to the patient with suspected hypereosinophilic syndrome. Hematology Am Soc Hematol Educ Program. 2022; 2022(1):47-54. doi: 10.1182/hematology.2022000367
2. Shomali W, Gotlib J. World Health Organization-Defined Eosinophilic Disorders: 2022 Update on Diagnosis, Risk Stratification, and Management. Am J Hematol. 2022;97(1):129-148. doi:10.1002/ajh.26352
Treatment of Eosinophilia
Sometimes glucocorticoids
If the eosinophilia is mild and there is no organ involvement, close observation with no treatment may be appropriate.
Medications known to be associated with eosinophilia are stopped. Asthma mediated by eosinophils can sometimes be treated with antibodies against IL-5 (eg, mepolizumab, reslizumab) or with antibodies against the IL-5 receptor such as benralizumab (1). Dupilumab, an IL-4/IL-13 inhibitor, may be used to treat chronic eosinophilic pneumonia and allergic bronchopulmonary aspergillosis (2).
If no cause is detected, the patient is followed for complications. A brief trial with low-dose glucocorticoids may lower the eosinophil count if eosinophilia is secondary (eg, to allergy, systemic rheumatic disease, or parasitic infection) rather than primary. Such a trial is indicated if eosinophilia is persistent and progressive in the absence of a treatable cause. Evaluation for Strongyloides infection in patients from tropical and subtropical regions is important because glucocorticoids can cause disseminated infection, which can be fatal. Because eosinophilia can involve multiple organ systems or may be a manifestation of a systemic disorder, multiple specialists may be needed for diagnostic and therapeutic input (3).
(See also Treatment of Hypereosinophilic Syndrome.)
Treatment references
1. Pelaia C, Calabrese C, Vatrell A, et al. Benralizumab: from the basic mechanism of action to the potential use in the biological therapy of severe eosinophilic asthma. Biomed Res Int. 2018;2018:4839230. doi:10.1155/2018/4839230
2. Eldaabossi SAM, Awad A, Anshasi N. Meprolizumab and dupliumab as a replacement to systemic glucocorticoids for the treatment of chronic eosinophilic pneumonia and allergic bronchopulmonary aspergillus-Case series, Almoosa specialist hospital. Respir Med Case Rep. 2021;34:201520. doi: 10.1016/j.rmcr.2021.101520
3. Thomsen GN, Christoffersen MN, Lindegaard HM, et al. The multidisciplinary approach to eosinophilia. Front Oncol. 2023;13:1193730. doi:10.3389/fonc.2023.1193730
Drug Information for the Topic





