

A brain abscess is an intracerebral collection of pus. Symptoms may include headache, lethargy, fever, and focal neurologic deficits. Diagnosis is by contrast-enhanced MRI or CT. Treatment is with antibiotics and usually CT-guided stereotactic aspiration or surgical drainage.
(See also Introduction to Brain Infections.)
An abscess forms when an area of cerebral inflammation becomes necrotic and encapsulated by glial cells and fibroblasts. Edema around the abscess may increase intracranial pressure, as may the abscess itself.
Etiology of Brain Abscess
A brain abscess can result from
Direct extension of cranial infections (eg, osteomyelitis, mastoiditis, sinusitis, subdural empyema)
Penetrating head wounds (including neurosurgical procedures)
Hematogenous spread (eg, in bacterial endocarditis [1], congenital heart disease with right-to-left shunt, or IV drug use)
Unknown causes
The bacteria involved are usually anaerobic and sometimes mixed, often including anaerobes, such as Bacteroides and anaerobic and microaerophilic streptococci. Staphylococci are commonly involved after cranial trauma, neurosurgery, or endocarditis. Enterobacteriaceae may be isolated in chronic ear infections. After chronic suppurative otitis media, anaerobic bacteria, streptococci, and gram-negative bacteria are common causes.
Fungi (eg, Aspergillus) and protozoa (eg, Toxoplasma gondii, particularly in patients with HIV infection) can cause abscesses.
Etiology reference
1. Bakshi R, Wright PD, Kinkel PR, et al: Cranial magnetic resonance imaging findings in bacterial endocarditis: The neuroimaging spectrum of septic brain embolization demonstrated in twelve patients. J Neuroimaging 9(2):78-84, 1999. doi: 10.1111/jon19999278
Symptoms and Signs of Brain Abscess
Symptoms result from increased intracranial pressure, mass effect, and sometimes focal brain injury. Classically, headache, nausea, vomiting, lethargy, seizures, personality changes, papilledema, and focal neurologic deficits develop over days to weeks; however, in some patients, these manifestations are subtle or absent until late in the clinical course.
Fever, chills, and leukocytosis may develop before the infection is encapsulated, but they may be absent at presentation, subside over time, or not develop.
Diagnosis of Brain Abscess
Contrast-enhanced MRI or, if unavailable, contrast-enhanced CT
When symptoms suggest an abscess, contrast-enhanced MRI with diffusion-weighted images or, if MRI is unavailable, contrast-enhanced CT is done. A fully developed abscess appears as an edematous mass with ring enhancement, which may be difficult to distinguish from a brain tumor or occasionally infarction; CT-guided aspiration, culture, surgical excision, or a combination may be necessary.
Culturing pus aspirated from the abscess can make targeted antibiotic therapy of the abscess possible. However, antibiotics should not be withheld until culture results are available.

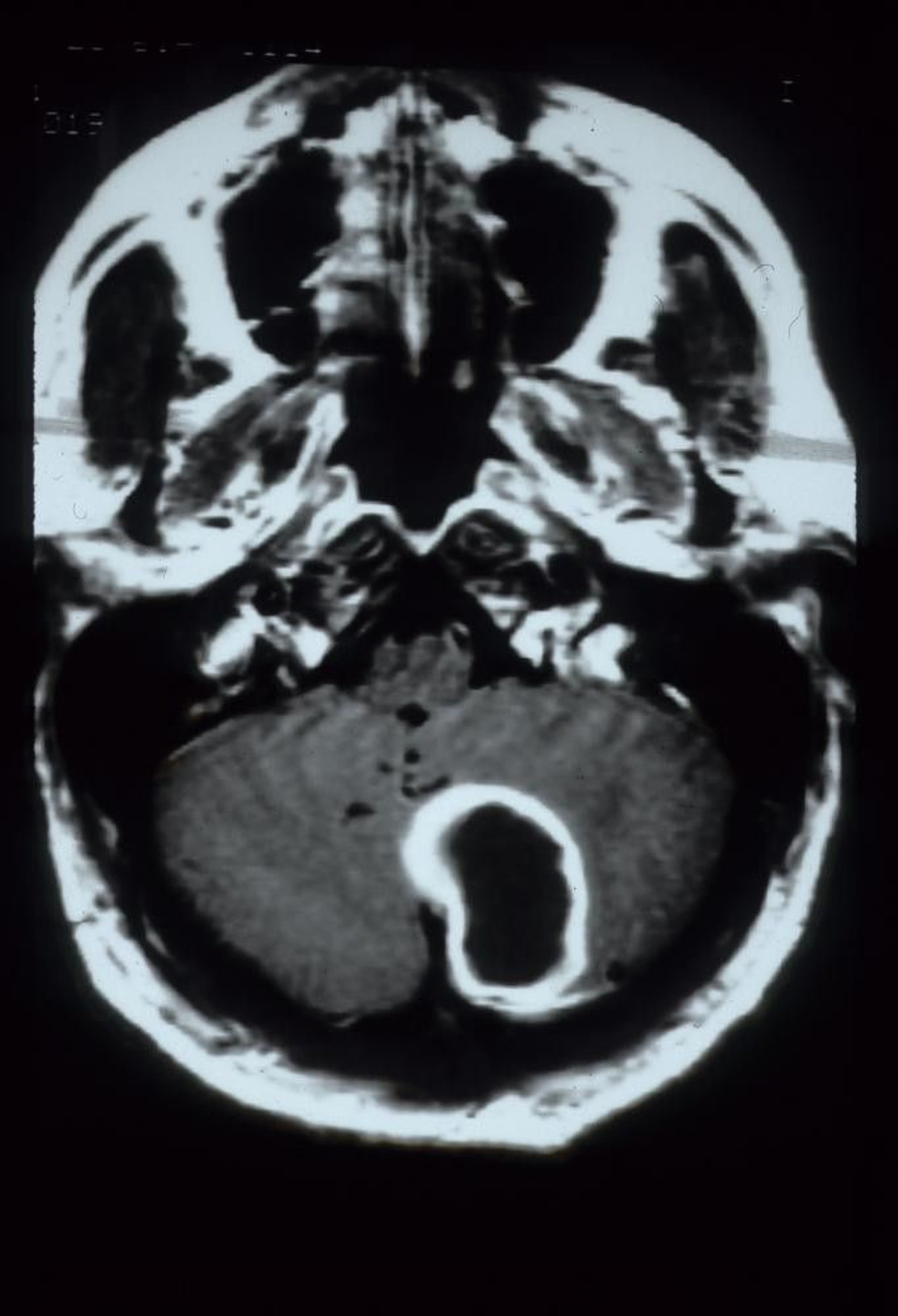
This gadolinium-enhanced MRI scan shows a cerebellar abscess, which appears as a large, rim-enhancing cavitary lesion in the left cerebellar hemisphere.
Courtesy of John E. Greenlee, MD.
Lumbar puncture is not done because it may precipitate transtentorial herniation and because cerebrospinal fluid (CSF) findings are nonspecific (see table ).
Treatment of Brain Abscess
Antibiotics (initially cefotaxime or ceftriaxone plus metronidazole for Antibiotics (initially cefotaxime or ceftriaxone plus metronidazole forBacteroides species or plus vancomycin for species or plus vancomycin forStaphylococcus aureus based on suspicion, then as guided by culture and susceptibility testing)
Usually CT-guided stereotactic aspiration or surgical drainage
Sometimes corticosteroids, antiseizure medications, or both
All patients receive antibiotics for a minimum of 4 to 8 weeks (1). Initial empiric antibiotics include one of the following:
CefotaximeCefotaxime
CeftriaxoneCeftriaxone
Both are effective against streptococci, Enterobacteriaceae, and most anaerobes but not against Bacteroides fragilis. If clinicians suspect Bacteroides species (as in chronic sinusitis or otitis), metronidazole is also required. If species (as in chronic sinusitis or otitis), metronidazole is also required. IfS. aureus is suspected (eg, after cranial trauma or neurosurgery or in endocarditis), vancomycin is used (with cefotaxime or ceftriaxone) until sensitivity to nafcillin is determined. Response to antibiotics is best monitored by serial MRI or CT.is suspected (eg, after cranial trauma or neurosurgery or in endocarditis), vancomycin is used (with cefotaxime or ceftriaxone) until sensitivity to nafcillin is determined. Response to antibiotics is best monitored by serial MRI or CT.
Drainage (CT-guided stereotactic or open) provides optimal therapy and is necessary for most abscesses that are solitary and surgically accessible, particularly those > 2 cm in diameter. If abscesses are < 2 cm in diameter, antibiotics alone may be tried, but abscesses must then be monitored with frequent serial MRI or CT (initially as often as every 2 to 3 days); if abscesses enlarge after being treated with antibiotics, surgical drainage is indicated.
Patients with increased intracranial pressure (assessed by signs and neuroimaging findings) may benefit from a short course of high-dose corticosteroids (dexamethasone 10 mg IV once, then 4 mg IV every 6 hours for 3 or 4 days).Patients with increased intracranial pressure (assessed by signs and neuroimaging findings) may benefit from a short course of high-dose corticosteroids (dexamethasone 10 mg IV once, then 4 mg IV every 6 hours for 3 or 4 days).
Antiseizure medications are frequently used to prevent seizures.
Rate of recovery depends on how successfully the abscesses are eradicated and the patient's immune status.
If immunocompromised patients (eg, patients with uncontrolled HIV infection) have an abscess due to Toxoplasma gondii or a fungus, they may have to take antibiotics for the rest of their life.
Treatment reference
1. Widdrington JD, Bond H, Schwab U, et al: Pyogenic brain abscess and subdural empyema: Presentation, management, and factors predicting outcome. Infection 46(6):785-792, 2018. doi: 10.1007/s15010-018-1182-9
Key Points
Brain abscess can result from direct extension (eg, of mastoiditis, osteomyelitis, sinusitis, or subdural empyema), penetrating wounds (including neurosurgery), or hematogenous spread.
Headache, nausea, vomiting, lethargy, seizures, personality changes, papilledema, and focal neurologic deficits develop over days to weeks; fever may be absent at presentation.
Do contrast-enhanced MRI or, if MRI is unavailable, contrast-enhanced CT.
Treat all brain abscesses with antibiotics (usually initially with ceftriaxone or cefotaxime plus metronidazole if clinicians suspect Treat all brain abscesses with antibiotics (usually initially with ceftriaxone or cefotaxime plus metronidazole if clinicians suspectBacteroides species or plus vancomycin if they suspect species or plus vancomycin if they suspectS. aureus), typically followed by CT-guided stereotactic aspiration or surgical drainage.
If abscesses are < 2 cm in diameter, they may be treated with antibiotics alone but must then be monitored closely with MRI or CT; if abscesses enlarge after being treated with antibiotics, surgical drainage is indicated.
Drug Information for the Topic





