



Snoring is a raspy noise produced in the nasopharynx during sleep. It is quite common, occurring in approximately 30% of men and 10% of women (1, 2); prevalence increases with age. However, because a bed partner's perception of and response to snoring is highly subjective and because snoring varies from night to night, prevalence estimates vary widely.
The sound ranges from barely audible to an extremely bothersome noise that may be loud enough to hear in another room. Usually, snoring is distressing to others (typically a bed partner or roommate trying to sleep) rather than the snorer; uncommonly, snorers wake up to the sound of their own snoring.
Snoring can have significant social consequences. It can cause strife between bed partners or roommates.
Other symptoms such as frequent awakenings, gasping or choking during sleep, excessive daytime sleepiness, and morning headaches may be present, depending on the severity, cause, and consequences of the snoring.


References
1. Kara CO, Zencir M, Topuz B, et al. The prevalence of snoring in adult population. Kulak Burun Bogaz Ihtis Derg. 14(1-2):18-24, 2005. Turkish.
2. Changsiripun C, Chirakalwasan N, Dias S, McDaid C. Management of primary snoring in adults: A scoping review examining interventions, outcomes and instruments used to assess clinical effects. Sleep Med Rev. 2024;77:101963. doi:10.1016/j.smrv.2024.101963.
Pathophysiology of Snoring
Snoring results from airflow-induced flutter of soft tissues of the nasopharynx, particularly the soft palate. As in any fluttering physical structure (eg, a flag), flutter in the nasopharynx develops depending on interacting factors, including the mass, stiffness, and attachments of the fluttering element and the velocity and direction of airflow.
The fact that people do not snore while awake suggests that sleep-induced muscular relaxation is at least part of the etiology because muscle tone is the only component of flutter that can change during sleep; tissue mass and attachments do not change. Furthermore, if pharyngeal dilators cannot keep the airway open in response to the negative intraluminal pressure induced by inspiration, the upper airway narrows, increasing local airflow velocity (for a given inspiratory volume). The increased flow velocity promotes flutter directly and decreases intraluminal pressure, further enhancing airway closure and thus promoting flutter and snoring.
Snoring is more likely to occur in the upper airway that is already compromised by structural factors, including
Micrognathia or retrognathia
Nasal septal deviation
Rhinitis that causes tissue swelling
Obesity
Macroglossia
Enlarged soft palate
Enlarged lateral pharyngeal walls
Etiology of Snoring
Primary snoring
Primary snoring is snoring that occurs in people who do not have excessive daytime sleepiness and that is not accompanied by awakening or excessive arousals, limitation of airflow, oxygen desaturation, or arrhythmias during sleep. Arousals are brief transitions to lighter sleep or awakenings that last < 15 seconds and are usually not noticed.
Sleep-disordered breathing
Snoring is usually a symptom of sleep-disordered breathing, which covers a spectrum ranging from upper airway resistance syndrome to obstructive sleep apnea (OSA). Each has similar upper airway obstructive pathophysiology but differs in degree and clinical consequences of the airway obstruction. The clinical consequences involve mainly disturbances of sleep and/or airflow.
Patients with obstructive sleep apnea have ≥ 5 episodes of apnea or hypopnea (with each episode lasting at least 10 seconds) per hour during sleep (apnea/hypopnea index [AHI]) plus ≥ 1 of the following (1):
Daytime sleepiness, unintentional sleep episodes, unrefreshing sleep, fatigue, or insomnia
Awakening with breath holding, gasping, or choking
Reports by a bed partner of loud snoring, breathing interruptions, or both during the patient's sleep
Obstructive sleep apnea can be categorized by severity:
Mild: 5 to 15 episodes/hour
Moderate: 16 to 30 episodes/hour
Severe: > 30 episodes/hour
Upper airway resistance syndrome (airflow limitation secondary to increased upper airway resistance or respiratory effort–related arousals [RERAs]) can cause excessive daytime sleepiness or other manifestations suggesting obstructive sleep apnea but with few episodes of apnea/hypopnea or oxygen desaturation; thus, it does not meet the criteria for obstructive sleep apnea.
Complications
Although snoring itself has no known adverse physiologic effects, obstructive sleep apnea may have consequences (eg, hypertension, stroke, heart disorders, atrial fibrillation).
Risk factors
Risk factors for snoring include
Older age
Obesity
Use of alcohol or other sedatives
Chronic nasal congestion or blockage
A small or posteriorly displaced jaw
Male sex
Postmenopausal status
Pregnancy
Abnormal structures that can block airflow (eg, large tonsils, a deviated nasal septum, nasal polyps, macroglossia, an enlarged soft palate, lateral pharyngeal narrowing)
There may also be familial risk.
Etiology reference
1. Kapur VK, Auckley DH, Chowdhuri S, et al. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. J Clin Sleep Med. 2017;13(3):479-504. Published 2017 Mar 15. doi:10.5664/jcsm.6506
Evaluation of Snoring
The primary goal is to identify snorers who are at high risk of having obstructive sleep apnea. Many snorers do not have OSA, but most patients with OSA snore (the precise proportion is not known).
Because several important manifestations of OSA are noticed mainly by others, bed partners or roommates should also be interviewed when possible.
History
History of present illness should cover severity of snoring, including its frequency, duration, and loudness. Also, the degree that snoring affects the bed partner should be noted.
Review of systems should seek symptoms suggesting obstructive sleep apnea, such as the presence of sleep disturbance as indicated by
Number of awakenings
Witnessed apneic or gasping/choking episodes
Presence of unrefreshing sleep or morning headaches
Excessive daytime sleepiness
The Epworth Sleepiness Scale can be used to quantify daytime sleepiness (1). The STOP-BANG score (see table STOP-BANG Risk Score for Obstructive Sleep Apnea) is a useful tool to predict risk of OSA for patients who snore (2).
STOP-BANG Risk Score for Obstructive Sleep Apnea
Item Evaluated | Finding |
|---|---|
Snoring | Loud snoring (louder than talking or loud enough to be heard through closed door) |
Tired | Often fatigue or sleepiness during the daytime |
Observed | Observed to stop breathing during sleep |
BP | High blood pressure or current treatment for hypertension |
BMI | > 35 kg/m2 |
Age | > 50 years |
Neck circumference | > 40 cm (> 15 3/4 in) |
Gender | Male |
≥ 3 or 4 findings = high risk of OSA. < 3 findings = low risk of OSA. | |
BMI = body mass index; OSA = obstructive sleep apnea. | |
Past medical history should note presence of disorders that may be associated with OSA, particularly hypertension, coronary ischemia, heart failure, stroke, gastroesophageal reflux disease (GERD), atrial fibrillation, depression, obesity (especially morbid obesity), and diabetes. Patients are asked how much alcohol they consume and when it is consumed in relation to bedtime. Medication and drug history may identify sedating or muscle-relaxing drugs.

Physical examination
Examination should begin by measuring height and weight, with calculation of body mass index (BMI).
The rest of the examination should focus on inspecting the nose and mouth for evidence of obstruction. Signs include
Nasal polyps and engorged turbinates
A high, narrow arched palate
Enlargement of the tongue, tonsils, soft palate, lateral pharyngeal walls, or uvula
A small or posteriorly displaced mandible (retrognathia)
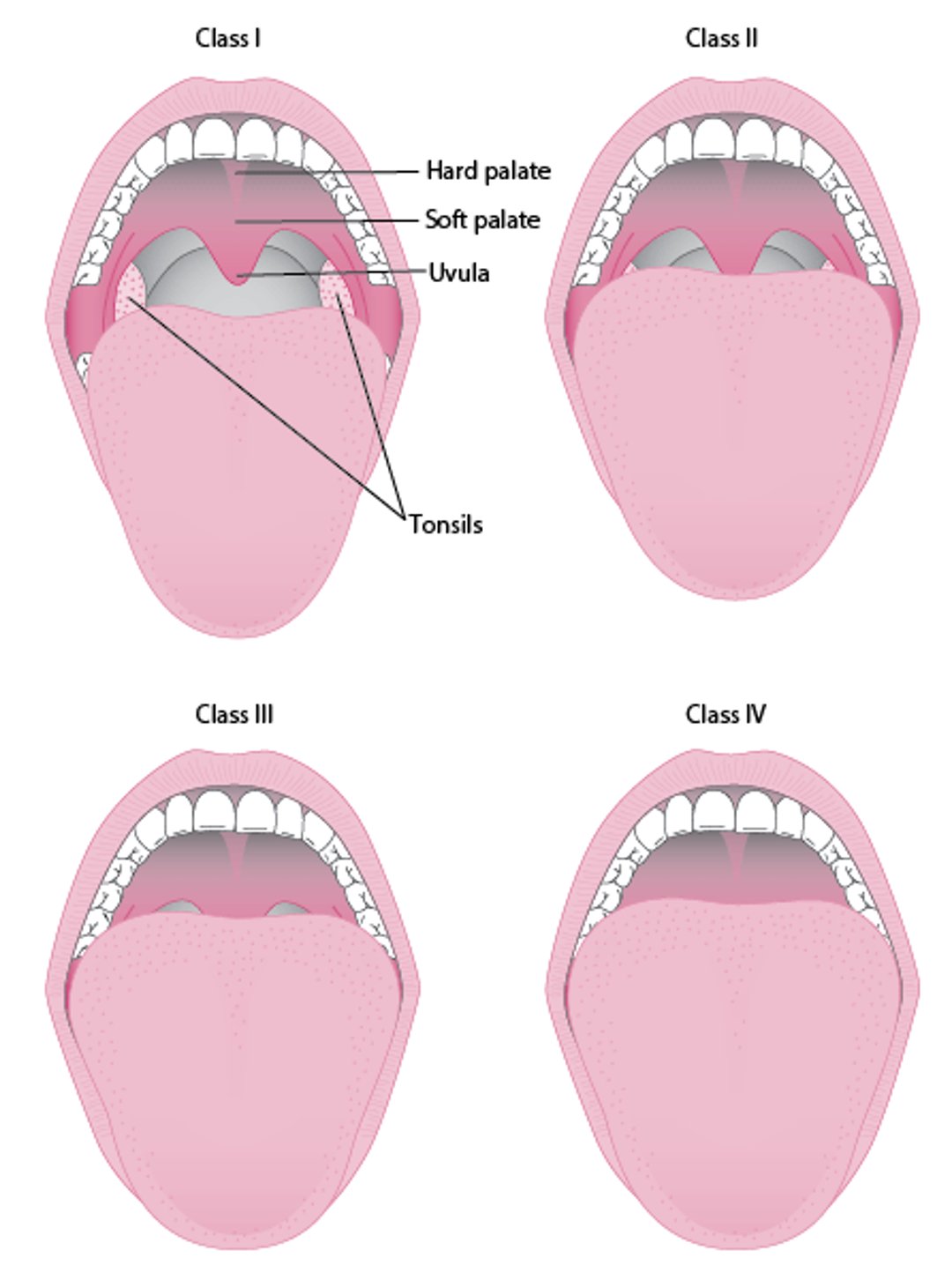
The Mallampati score is a tool for airway assessment based on oropharyngeal visibility, and is widely used in anesthesiology for evaluating intubation feasibility. A modified Mallampati score of 3 or 4 (only the base or none of the uvula is visible during oral inspection—see figure Mallampati Scoring) suggests increased risk of OSA.
Modified Mallampati Scoring
Modified Mallampati scoring is as follows:
|

Red flags
The following findings are of particular concern:
Witnessed apnea or choking during sleep
Morning headaches
Epworth sleepiness score ≥ 10
BMI ≥ 35 kg/m2
Very loud, constant snoring
Interpretation of findings
The clinical evaluation is not completely reliable for diagnosis of obstructive sleep apnea but can be suggestive. Red flag findings clearly correlate with OSA. However, all of these findings occur along a continuum, and there is no widespread agreement on cut-off points and relative weighting. Nonetheless, the more red flag findings a patient has and the more severe they are, the greater the likelihood of OSA.
Testing
Testing for OSA is by polysomnography (in a laboratory) or with a home sleep apnea study. An in-laboratory sleep study monitors brain activity (via EEG), eye movements, heart rate, nasal pressure, chest and abdominal wall movement, oxygen saturation, EEG arousals, muscle tone, snoring, EKG, body position, CO2, and activity (including periodic limb movements) during sleep. Home sleep studies typically monitor nasal pressure, chest or abdominal motion, oxygen saturation, snoring, and body position. Thus, in most patients complaining of only snoring, home sleep studies (which are readily available) can be performed.
Evaluation references
1. Boyes J, Drakatos P, Jarrold I, Smith J, Steier J. The use of an online Epworth Sleepiness Scale to assess excessive daytime sleepiness. Sleep Breath. 2017;21(2):333-340. doi:10.1007/s11325-016-1417-x
2. Chung F, Subramanyam R, Liao P, Sasaki E, Shapiro C, Sun Y. High STOP-Bang score indicates a high probability of obstructive sleep apnoea. Br J Anaesth. 2012;108(5):768-775. doi:10.1093/bja/aes022
Treatment of Snoring
Treatment of snoring associated with other conditions, such as chronic nasal obstruction and obstructive sleep apnea, are discussed elsewhere in The Manual.
Overall, treatment includes general measures to manage risk factors plus physical methods to open the upper airway and/or stiffen the involved structures.
General measures
Several general measures can be used for primary snoring. Their efficacy has not been well-evaluated, primarily because perception of snoring is highly subjective. Measures include
Avoiding alcohol and sedating drugs for several hours before bedtime
Sleeping with the head elevated (best accomplished by using bed- or body-positioning devices such as wedges) or sleeping in the lateral decubitus position
Weight loss if overweight/obesity is a concern (consider a glucagon-like peptide [GLP]-1 agonist)
Treating any nasal congestion (eg, with a glucocorticoid spray)
The best way to elevate the head is to put blocks under 2 of the bed's legs to raise the head of the bed or to use a wedge pillow that slants the whole upper body. People should not use pillows to raise only the head.
Measures that force the sleeper onto his/her side during the night could include, for example, attaching a tennis ball to the back of a person's night shirt.
Bed partners may benefit from using earplugs or white-noise machines. Sometimes alternate sleeping arrangements (eg, separate rooms) are necessary.
Oral appliances
Oral appliances are worn only during sleep; they include
Mandibular advancement devices
Tongue-retaining devices
These appliances should be fitted by specially trained dentists. They are helpful for patients with OSA and are generally regarded as effective for simple snoring, although studies in this area are scant.
Adverse effects include temporomandibular joint (TMJ) discomfort, dental misalignment, and excessive salivation, but most patients tolerate the devices well.
Mandibular advancement devices are most commonly used. These devices, which are made by specially qualified dentists, move the mandible and tongue forward relative to the maxilla and thus increase airway caliber during sleep. Most can be adjusted incrementally after the initial fitting to optimize results (unlike "boil-and-bite" self-fitted appliances that can be bought over-the-counter).
Tongue-retaining devices use suction to maintain the tongue in an anterior position. Tongue-retaining devices are more uncomfortable than mandibular advancement devices.
A removable tongue muscle stimulator is designed to be used during the day and to improve tongue muscle function in patients with snoring or OSA.
Continuous positive airway pressure (CPAP)
CPAP devices maintain a constant positive pressure in the upper airway via a small mask applied to the nose or nose and mouth. By increasing the caliber of the upper airway, CPAP prevents narrowing or collapse of the upper airway during sleep. It thus is very effective for OSA and is effective for primary snoring. However, patients may have difficulty tolerating CPAP. Although patients are often willing to use a CPAP device nightly to avoid the significant symptoms and long-term consequences of OSA, they are less willing to use the device to manage primary snoring, whose consequences are primarily social. In the United States, third-party reimbursement typically does not cover CPAP for snoring.
Surgery
Because reduced nasal patency promotes snoring, surgically correcting specific causes of airway compromise (eg, nasal polyps, hypertrophied tonsils, deviated septum) may be a reasonable way to decrease snoring. However, studies have not yet demonstrated significant benefit (1).
Various pharyngeal surgical procedures that alter the structure of the palate and sometimes the uvula have been developed for obstructive sleep apnea. Some are also useful for nonapneic snoring.
Uvulopalatopharyngoplasty involves remodeling the uvula, palate, and pharyngeal walls to increase the size of the airway. It can be effective for snoring, although effects may not last beyond a few years (2). It is an inpatient procedure requiring general anesthesia; thus, its justification for snoring alone is limited (3). It is also now used less frequently than procedures that are less aggressive.
Therefore, a number of outpatient palate-altering procedures requiring only a local anesthetic have been developed:
Laser-assisted uvuloplasty is less invasive than uvulopalatopharyngoplasty. Although some patients report benefit, benefits tend to wane over time (4) and its long-term usefulness in treating snoring has not been proved.
For injection snoreplasty, a sclerotherapeutic agent is injected into the submucosa of the soft palate to stiffen it and the uvula. Its usefulness for snoring alone requires further study.
For radiofrequency ablation, a probe is used to introduce thermal energy into the soft palate. Small studies have shown its usefulness for snoring, but further study is needed.
Palatal implants, made of polyethylene, can be placed into the soft palate to stiffen it. Three or more small implants are used. Their usefulness for snoring alone has not been proved (5), and the implants can extrude.
Treatment references
1. Sundaram S, Bridgman SA, Lim J, Lasserson TJ. Surgery for obstructive sleep apnoea. Cochrane Database Syst Rev. 2005;2005(4):CD001004. Published 2005 Oct 19. doi:10.1002/14651858.CD001004.pub2
2. Hicklin LA, Tostevin P, Dasan S. Retrospective survey of long-term results and patient satisfaction with uvulopalatopharyngoplasty for snoring. J Laryngol Otol. 114(9):675-681, 2000. doi: 10.1258/0022215001906697
3. Camacho M, Guilleminault C, Wei JM, et al. Oropharyngeal and tongue exercises (myofunctional therapy) for snoring: a systematic review and meta-analysis. Eur Arch Otorhinolaryngol. 275(4):849-885, 2018. doi: 10.1007/s00405-017-4848-5
4. Iyngkaran T, Kanagalingam J, Rajeswaran R, et al. Long-term outcomes of laser-assisted uvulopalatoplasty in 168 patients with snoring. J Laryngol Otol. 120(11):932-938, 2006. doi: 10.1017/S002221510600209X
5. Choi JH, Cho JH, Chung YS, et al. Effect of the Pillar implant on snoring and mild obstructive sleep apnea: A multicenter study in Korea. Laryngoscope. 125(5):1239-1243, 2015. doi: 10.1002/lary.24975
Key Points
Only some patients who snore have obstructive sleep apnea (OSA), but most patients who have OSA snore.
Clinical risk factors such as nocturnal apneic or choking episodes, daytime sleepiness, and a high BMI help identify patients at risk of OSA and thus in need of testing with polysomnography or home sleep studies.
Recommend general measures to reduce snoring (eg, avoiding alcohol and sedating drugs, sleeping with the head elevated or in the lateral decubitus position, losing weight with a GLP-1 agonist).
Consider specific measures such as mandibular advancement devices, palate-altering procedures, and CPAP to treat snoring due to OSA.
Drug Information for the Topic





