





Neural tube defects are a certain type of birth defect of the brain, spine, and/or spinal cord.
Neural tube defects can result in nerve damage, learning disabilities, paralysis, and death.
The diagnosis can be made before birth and is based on a blood test, an amniotic fluid test, or an ultrasound.
After birth, doctors do a physical examination and may do additional imaging tests.
Surgery usually is needed to close neural tube defects.
Folate (folic acid) taken by the mother before conception and during the first trimester can help prevent these defects.
In the fetus, the brain and spinal cord develop as a groove that folds over to become a tube called the neural tube. Layers of tissue that come from this tube normally become the brain and spinal cord and the tissues that cover them, including part of the spine and the meninges. Sometimes the neural tube does not develop normally, which may affect the brain, spinal cord, and meninges.
Spina Bifida
Spina bifida is a neural tube defect. Although spina bifida can be serious, people who have it may live a long life.
Spina bifida results when the neural tube fails to close completely and remains an open channel. In spina bifida, the bones of the spine or backbone (vertebrae) do not close over and protect the spinal cord. The spine in the lower back is most commonly affected. One or more of the vertebrae may be involved.
Spina bifida occulta is the mildest form of spina bifida. Typically, only some of the bones of the spine are affected, and the spinal cord and meninges are unaffected.
This common defect is called "occulta" because it is hidden (covered) by a layer of skin. This skin layer typically appears normal, but sometimes it is a different color than the surrounding skin, or there may be a small tuft of hair over the area.
Spina bifida occulta usually causes no symptoms, but children who are initially thought to have it may have other birth defects or abnormalities of the spinal cord (occult spinal dysraphism).
Occult spinal dysraphism is a form of spina bifida in which the spinal cord is affected. In occult spinal dysraphism, newborns may have visible skin abnormalities on their lower back. These include birthmarks, overly pigmented areas (hemangiomas and flame nevus [stork bite]), tufts of hair, openings in the skin (dermal sinus tract), a deep dimple or pit in the lower back above the crease of the buttocks, or small lumps (masses). The underlying spinal cord may have a defect, such as a fatty tumor (lipoma), or the band that anchors the spinal cord (filum terminale) may be thickened and short, causing the cord to be stretched and unable to move normally within the spinal canal (called tethering). As the child grows, the spinal cord must be able to move freely inside the spinal canal. If not treated, tethering can lead to nerve damage that results in a loss of bladder and bowel control, leg weakness, and spasm of leg muscles, which can eventually lead to an inability to walk.
Spina bifida cystica is the most serious form of spina bifida. In spina bifida cystica, tissues of the meninges, spinal cord, or both push through the opening in the vertebrae and bulge out in a sac from the baby's back. A thin membrane of skin may cover the sac, or the sac may not be covered by skin.
The sacs are named by what tissues they contain:
A meningocele: Contains only the meninges
A meningoencephalocele: Contains the meninges and brain tissue
A myelomeningocele: Contains the meninges and spinal cord tissue
An encephalocele: Contains only brain tissue
A myelocele: Contains only spinal cord tissue
Damage to brain or spinal cord tissue is much more likely when the sac bulges outside the normal contour of the back, especially if there is no normal skin covering it. The sac can easily burst open, so when spinal cord tissue or meninges are fully exposed, they may become infected by bacteria, causing meningitis.
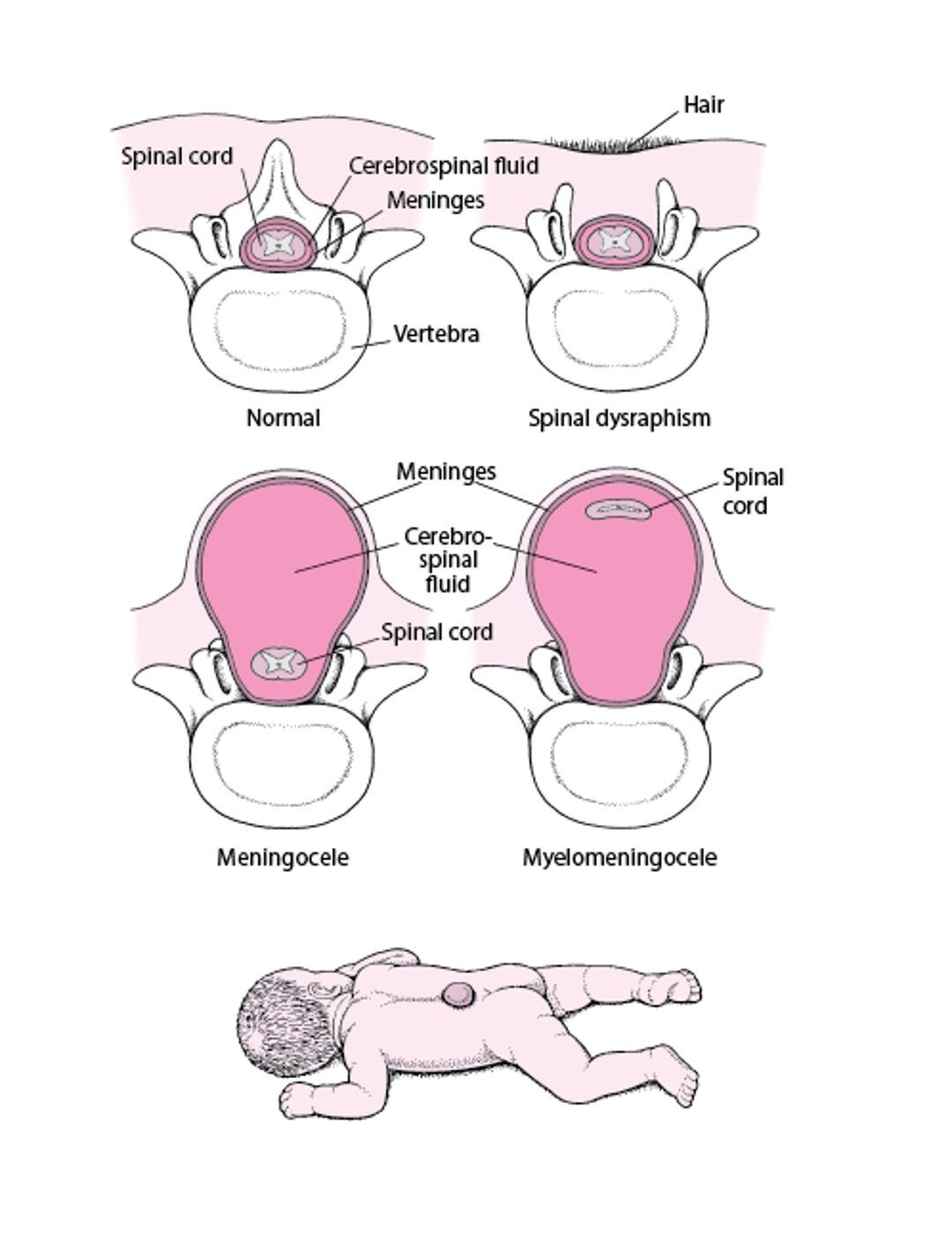
Spina Bifida: A Defect of the Spine
In spina bifida, the bones of the spine (vertebrae) do not form normally. Spina bifida can vary in severity. In occult spinal dysraphism, one or more vertebrae do not form normally, and the spinal cord and the layers of tissues (meninges) surrounding it may also be affected. There are several types with differing neurologic severities. The diagnosis is sometimes suggested by symptoms in the lower back, such as a tuft of hair, a dimple or pit, or a pigmented area on the skin over the defect. In a meningocele, the meninges push through the incompletely formed vertebrae, resulting in a fluid-filled bulge under the skin. The spinal cord is in its normal location. The most severe type is a myelomeningocele, in which the meninges and spinal cord bulge out in a sac from the baby's back. In a myelomeningocele, the meninges are usually exposed or, rarely, are covered by a thin layer of skin (as shown in the figure). The affected area appears raw and red, and the baby is likely to be severely impaired. |

Other neural tube and associated defects
Anencephaly is the most severe neural tube defect. In anencephaly, the brain tissue does not develop. This defect is always fatal.
Chiari malformation may occur in many children with spina bifida. This defect causes the cerebellum (the part of the brain that controls balance) to be pushed downward through the opening at the bottom of the skull where the brain and spinal cord connect. The protruding cerebellum may put pressure on the brain stem or spinal cord. Children may develop hydrocephalus (fluid on the brain) because the pressure from the cerebellum may block the flow of fluid in and around the brain.
Syringomyelia occurs when the normally small fluid-filled central canal within the spinal cord widens and fills with a larger amount of fluid. Syringomyelia can occur with spina bifida or with Chiari malformations and can make people less sensitive to pain and temperature changes over the shoulders, neck, and arms.
Causes of Neural Tube Defects
There are many causes of neural tube defects.
Deficiency of a B vitamin, folate, during pregnancy is a significant factor.
Genetic factors may play a role. Use of certain medications by the mother during pregnancy (such as valproate) and diabetes in the mother are risk factors for neural tube defects. The defect often develops before the mother knows she is pregnant.
Symptoms of Neural Tube Defects
Many children who have minor neural tube defects have no symptoms.
Most symptoms caused by neural tube defects result from brain or spinal cord damage.
Neural tube defects can cause brain damage, hydrocephalus, learning disabilities, and difficulty swallowing.
Spinal cord damage can cause severe problems, typically involving the bowels, bladder, and legs. Problems include:
Weakness and paralysis: Walking can be difficult or impossible, unused muscles shrink and stiffen up
Decreased sensation of the skin
Urinary problems: Inability to pass urine (urine retention) or urinary incontinence and frequent urinary tract infections (severe urinary problems sometimes lead to kidney failure)
Bowel problems: Loss of control over bowel movements or constipation
Other problems, such as clubfoot, arthrogryposis (joints, usually ankles, that become frozen and cannot bend), a dislocated hip, or an abnormally curved spine that causes a humpback (kyphosis), may also be present at birth. Scoliosis may develop later in some children.
Diagnosis of Neural Tube Defects
Before birth, blood tests or amniocentesis to measure alpha-fetoprotein levels, or prenatal ultrasounds
After birth, physical examination and additional imaging tests
Many neural tube defects can be detected before birth with prenatal screening tests.
A high level of alpha-fetoprotein in a pregnant person's blood or in amniotic fluid may indicate a neural tube defect in the fetus. So during the second trimester, blood tests or amniocentesis (removing a sample of fluid from around the fetus) may be done to measure these levels.
Before birth, prenatal ultrasounds may show the defect or characteristic abnormalities.
After birth, some defects are obvious during the physical examination. If newborns have abnormalities that suggest occult spinal dysraphism, ultrasound or magnetic resonance imaging (MRI) is done to check for defects in the spine. X-rays of the spine, hips, and sometimes the legs are done.
After spina bifida is diagnosed, tests to evaluate bladder function are done. They include urinalysis, urine culture, blood tests, and ultrasounds.
Treatment of Neural Tube Defects
Surgery
Health care professionals, usually a team of specialists that includes a neurosurgeon, a urologist, a pediatrician, a pediatric rehabilitation medicine specialist, an orthopedic surgeon, a physical therapist, a nurse practitioner, and a social worker, evaluate the type and severity of the defect and talk to the family about how treatment and care can be implemented.
Neural tube defects are usually closed surgically. Certain defects, such as a myelomeningocele, are typically repaired soon after birth. Some defects can be repaired during pregnancy before the baby is born.
A shunt (a plastic tube that creates a permanent alternate drainage path for cerebrospinal fluid) may be placed to treat hydrocephalus.
Problems with the bladder, bones, or muscles and other problems are treated as needed.
Prognosis for Neural Tube Defects
With appropriate care, most children do well.
However, complications, such as loss of kidney function and problems with shunts needed to treat hydrocephalus, may occur and sometimes are fatal in older children.
Prevention of Neural Tube Defects
Folate
Folate reduces the risk of neural tube defects.
To prevent a neural tube defect in a fetus (and child), all people who are planning to become pregnant or may become pregnant should take a vitamin supplement with folic acid (folate), ideally beginning 3 months before getting pregnant and continuing through the first trimester of pregnancy.
For women who have not had a fetus with a neural tube defect, the recommended daily dose of folate is 400 to 800 mcg (0.4 to 0. 8 mg). Women who have had an infant with a neural tube defect are at high risk of having another affected infant and should take a higher daily dose of folate, 4000 mcg (4 mg). Folate supplements may not prevent all neural tube defects in future pregnancies but can reduce the risk of neural tube defects substantially.
Did You Know...
|
More Information
The following English-language resources may be useful. Please note that The Manual is not responsible for the content of these resources.
Drug Information for the Topic





