



Cardiac imaging tests can delineate cardiac structure and function. Standard imaging tests include:
Computed tomography (CT) and CT angiography
Magnetic resonance imaging (MRI) and MR angiography
Echocardiography is discussed separately.
Standard CT and MRI have limited application because the heart constantly beats, but faster CT and magnetic resonance techniques can provide useful cardiac images if the rhythm is regular and the heart rate is controlled; sometimes patients are given a medication (eg, a beta-blocker) to slow the heart rate during imaging.
In ECG gating, the image recording (or reconstruction) is synchronized with the electrocardiogram (ECG), providing information from several cardiac cycles that can be used to create single images of selected points in the cardiac cycle. CT gating is a form of ECG gating that uses the ECG to trigger the x-ray beam at the desired portion of the cardiac cycle, exposing the patient to less radiation than gating that reconstructs information from only the desired portion of the cardiac cycle (gated reconstruction) and does not interrupt the x-ray beam.
Chest Radiography in Cardiac Diagnosis
Chest radiographs are often useful as a starting point in a cardiac diagnosis. They are often performed in the evaluation of symptoms that might be cardiac in origin (eg, chest pain) and can provide valuable anatomic information, although additional tests are almost always required for precise characterization of cardiac structure and function. Posteroanterior and lateral views provide a gross view of atrial and ventricular size and shape, pulmonary vasculature, bronchial anatomy, and aortic arch-sidedness. A chest radiograph should always be performed when a diagnosis of heart failure is considered.

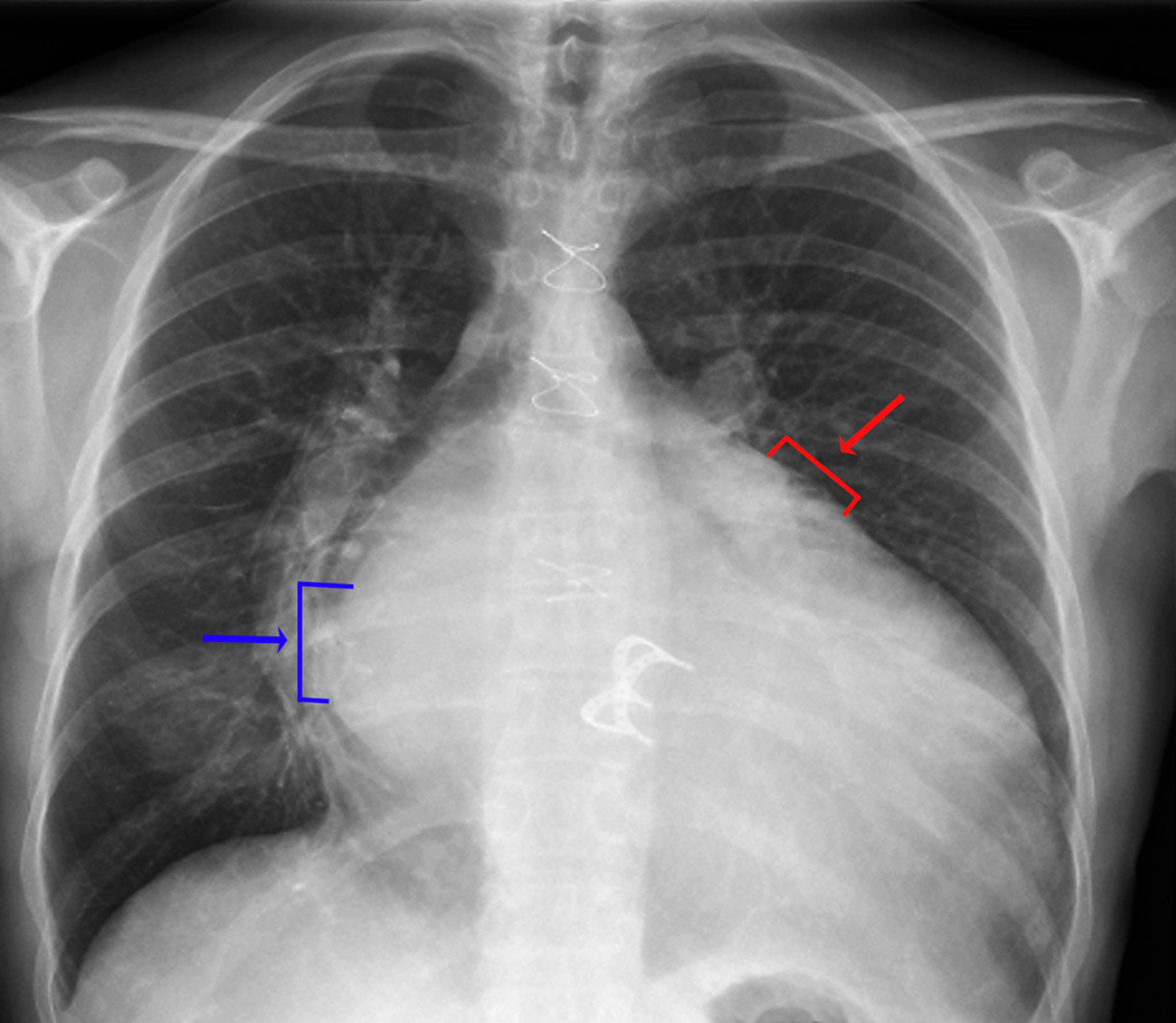
Signs of left atrial enlargement include a visible density of the left atrium in the right hemithorax (blue arrow, double-density sign), increased (> 7 cm) distance between the left atrial edge in the right hemithorax and the left mainstem bronchus, a convexity along the upper left heart border caused by enlargement of the left atrial appendage (red arrow), and widening of the carina with increased separation between the left and right mainstem bronchi. Signs of left ventricular enlargement include an obvious enlargement of the cardiac silhouette and leftward and inferior displacement of the left heart border.
ZEPHYR/SCIENCE PHOTO LIBRARY
Computed Tomography (CT) in Cardiac Diagnosis
CT may be used to evaluate for pericarditis, congenital cardiac disorders (especially abnormal arteriovenous connections), disorders of the great vessels (eg, aortic aneurysm, aortic dissection), cardiac tumors, acute pulmonary embolism, chronic pulmonary thromboembolic disease, and arrhythmogenic right ventricular cardiomyopathy. Noncontrast CT can be used to look for coronary artery calcification; the calcium load is sometimes used to refine estimates of cardiac risk. The use of CT to evaluate most other cardiac conditions, particularly those involving blood vessels, requires a radiopaque contrast agent, which may limit its use in patients with renal impairment. When used to image blood vessels specifically, CT with contrast is termed CT angiography and is often ECG-gated.
Coronary CT angiography (CCTA), a noninvasive alternative to coronary angiography, relies on multidetector CT technology. CCTA, is especially used for patients with chest pain and a low to intermediate probability of acute coronary syndrome (1). When used with beta-blockade to slow the heart rate and nitroglycerin to dilate the coronary arteries, it is up to 97% sensitive for significant obstructive coronary artery disease (2). Radiation levels are reasonable (1 to 10 mSv, compared with average annual background radiation exposure of 3.6 mSv) with current imaging protocols, including prospective ECG-gating (3). However, the presence of high-density calcified plaques creates imaging artifacts that interfere with interpretation. CCTA can be combined with a noninvasive estimate of fractional flow reserve (FFR), an important parameter in evaluating the functional hemodynamic significance of coronary lesions, and which otherwise requires invasive assessment in the cardiac catheterization laboratory (4).


Cross sectional view of a cardiac CT angiogram shows the left ventricle and the left anterior descending coronary artery.
LIVING ART ENTERPRISES, LLC/SCIENCE PHOTO LIBRARY

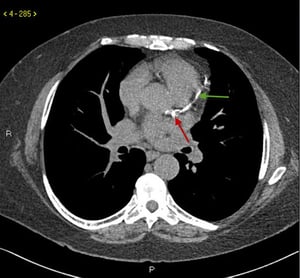
This image shows dense coronary calcifications in the left main (red arrow) and left anterior descending coronary artery (green arrow).
This image shows dense coronary calcifications in the left main (red arrow) and left anterior descending coronary arter
© 2017 Elliot K. Fishman, MD.

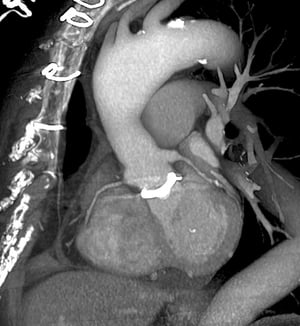
This is an oblique view of the left side, looking toward the front of the chest (left). The prosthetic heart valve (white) is visible at center, where the aorta (upper center) meets the heart (lower center). The stitches used to close the chest are visible at upper left. The 3D appearance is achieved through computerized reconstruction of multiple single-plane images.
This is an oblique view of the left side, looking toward the front of the chest (left). The prosthetic heart valve (whi
ZEPHYR/SCIENCE PHOTO LIBRARY
This image shows dense coronary calcifications in the left main (red arrow) and left anterior descending coronary artery (green arrow).
This image shows dense coronary calcifications in the left main (red arrow) and left anterior descending coronary arter
© 2017 Elliot K. Fishman, MD.
This is an oblique view of the left side, looking toward the front of the chest (left). The prosthetic heart valve (white) is visible at center, where the aorta (upper center) meets the heart (lower center). The stitches used to close the chest are visible at upper left. The 3D appearance is achieved through computerized reconstruction of multiple single-plane images.
This is an oblique view of the left side, looking toward the front of the chest (left). The prosthetic heart valve (whi
ZEPHYR/SCIENCE PHOTO LIBRARY

This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descending and left circumflex arteries are indicated by the green and blue arrows respectively and the right coronary artery is indicated by the purple arrow. (Not all arteries are seen in all images.) In this image, the origin of the left coronary artery is visible.
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descend
© 2017 Elliot K. Fishman, MD.
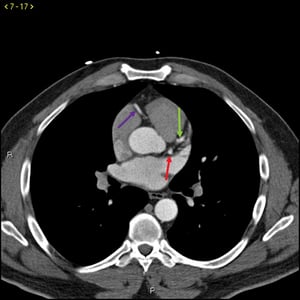
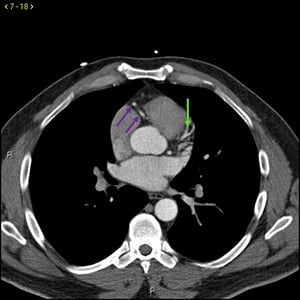
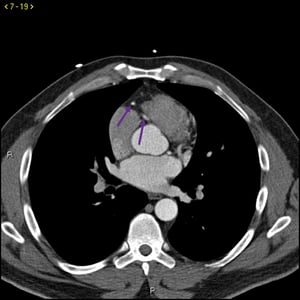
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descending and left circumflex arteries are indicated by the green and blue arrows, respectively, and the right coronary artery is indicated by the purple arrow. (Not all arteries are seen in all images.)
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descend
© 2017 Elliot K. Fishman, MD.
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descending and left circumflex arteries are indicated by the green and blue arrows respectively and the right coronary artery is indicated by the purple arrow. (Not all arteries are seen in all images.)
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descend
© 2017 Elliot K. Fishman, MD.
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descending and left circumflex arteries are indicated by the green and blue arrows respectively and the right coronary artery is indicated by the purple arrow. (Not all arteries are seen in all images.)
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descend
© 2017 Elliot K. Fishman, MD.
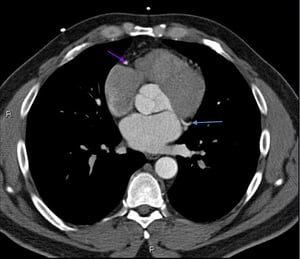
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descending and left circumflex arteries are indicated by the green and blue arrows respectively and the right coronary artery is indicated by the purple arrow. (Not all arteries are seen in all images.) In this image, the origin of the right coronary artery is visible.
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descend
© 2017 Elliot K. Fishman, MD.

This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descending and left circumflex arteries are indicated by the green and blue arrows respectively and the right coronary artery is indicated by the purple arrow. (Not all arteries are seen in all images.)
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descend
© 2017 Elliot K. Fishman, MD.
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descending and left circumflex arteries are indicated by the green and blue arrows respectively and the right coronary artery is indicated by the purple arrow. (Not all arteries are seen in all images.) In this image, the origin of the left coronary artery is visible.
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descend
© 2017 Elliot K. Fishman, MD.
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descending and left circumflex arteries are indicated by the green and blue arrows, respectively, and the right coronary artery is indicated by the purple arrow. (Not all arteries are seen in all images.)
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descend
© 2017 Elliot K. Fishman, MD.
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descending and left circumflex arteries are indicated by the green and blue arrows respectively and the right coronary artery is indicated by the purple arrow. (Not all arteries are seen in all images.)
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descend
© 2017 Elliot K. Fishman, MD.
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descending and left circumflex arteries are indicated by the green and blue arrows respectively and the right coronary artery is indicated by the purple arrow. (Not all arteries are seen in all images.)
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descend
© 2017 Elliot K. Fishman, MD.
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descending and left circumflex arteries are indicated by the green and blue arrows respectively and the right coronary artery is indicated by the purple arrow. (Not all arteries are seen in all images.) In this image, the origin of the right coronary artery is visible.
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descend
© 2017 Elliot K. Fishman, MD.
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descending and left circumflex arteries are indicated by the green and blue arrows respectively and the right coronary artery is indicated by the purple arrow. (Not all arteries are seen in all images.)
This contrast CT shows normal coronary arteries. The left main is indicated by the red arrow. The left anterior descend
© 2017 Elliot K. Fishman, MD.

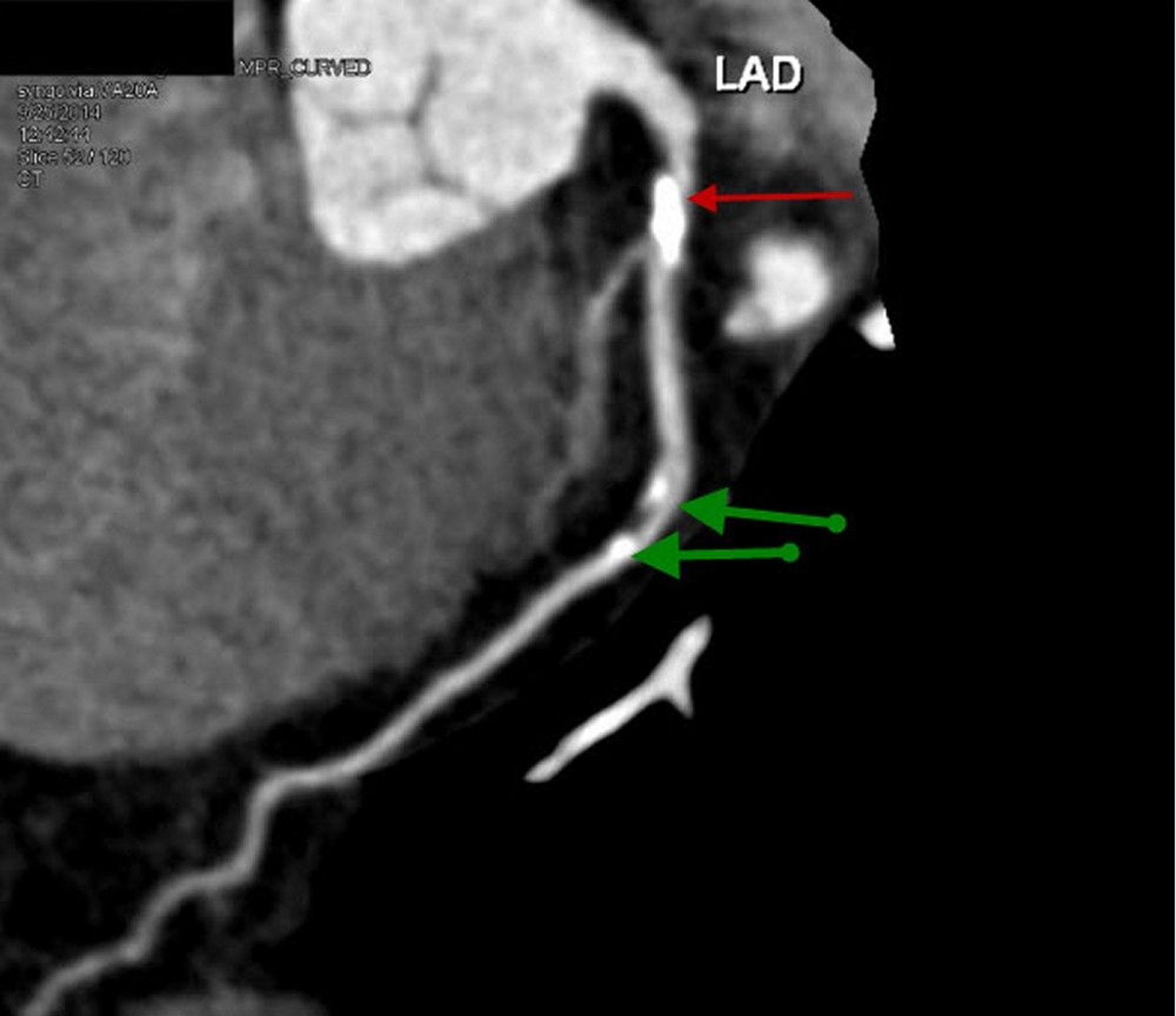
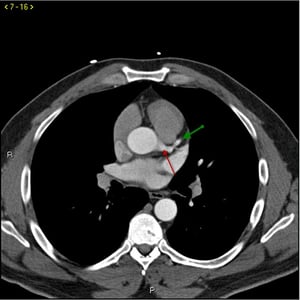
This contrast CT shows a reconstructed sagittal view of proximal left anterior descending (LAD) artery with prominent calcified plaque and 70% stenosis (red arrow). Mid LAD shows mild stenosis of 20–30% (green arrows).
© 2017 Elliot K. Fishman, MD.
Coronary calcium scoring, using nonenhanced scans to evaluate for coronary artery calcification, are also an important tool in risk stratification. The amount of coronary artery calcium present can be used to determine the 10-year risk of coronary artery disease (see The Multi-Ethnic Study of Atherosclerosis (MESA) risk calculator). The absence of coronary artery calcium portends a very favorable prognosis (5, 6, 7). (See also Calcium Scoring CT.)
CT in cardiac diagnosis references
1. Gulati M, Levy PD, Mukherjee D, et al. 2021 AHA/ACC/ASE/CHEST/SAEM/SCCT/SCMR Guideline for the Evaluation and Diagnosis of Chest Pain: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;144(22):e368-e454. doi:10.1161/CIR.0000000000001029
2. Joshi PH, de Lemos JA. Diagnosis and Management of Stable Angina: A Review. JAMA. 2021;325(17):1765-1778. doi:10.1001/jama.2021.1527
3. Abbara S, Blanke P, Maroules CD, et al. SCCT guidelines for the performance and acquisition of coronary computed tomographic angiography: A report of the Society of Cardiovascular Computed Tomography Guidelines Committee: Endorsed by the North American Society for Cardiovascular Imaging (NASCI). J Cardiovasc Comput Tomogr. 2016;10(6):435-449. doi:10.1016/j.jcct.2016.10.002
4. Slipczuk L, Blankstein R, Bucciarelli-Ducci C, et al. State of the Art: Evaluation and Medical Management of Nonobstructive Coronary Artery Disease in Patients With Chest Pain: A Scientific Statement From the American Heart Association. Circulation. 2025;152(23):e443-e466. doi:10.1161/CIR.0000000000001394
5. Blaha M, Budoff MJ, Shaw LJ, et al. Absence of coronary artery calcification and all-cause mortality. JACC Cardiovasc Imaging. 2009;2(6):692-700. doi:10.1016/j.jcmg.2009.03.009
6. Grandhi GR, Mszar R, Cainzos-Achirica M, et al. Coronary Calcium to Rule Out Obstructive Coronary Artery Disease in Patients With Acute Chest Pain. JACC Cardiovasc Imaging. 2022;15(2):271-280. doi:10.1016/j.jcmg.2021.06.027
7. Sarwar A, Shaw LJ, Shapiro MD, et al. Diagnostic and prognostic value of absence of coronary artery calcification. JACC Cardiovasc Imaging. 2009;2(6):675-688. doi:10.1016/j.jcmg.2008.12.031
Cardiac Magnetic Resonance Imaging (MRI)
Standard MRI is useful for evaluating areas around the heart, particularly the mediastinum and great vessels (eg, for studying aneurysms, dissections, congenital heart disease, and stenoses). With ECG-gated data acquisition, cardiac MRI can be used to image the heart itself, and it has better soft-tissue resolution than that of CT or echocardiography, clearly delineating myocardial wall thickness and motion, chamber volumes, intraluminal masses or clot, and valve planes. MRI can be used to quantify left and right ventricular volumes and ejection fraction when echocardiography is inadequate or unsuitable. MRI carries the advantage over CT of not exposing the patient to ionizing radiation. Cardiac MRI can also quantify the ratio of pulmonary to systemic blood flow, the ratio of right to left pulmonary blood flow, blood flow across specific vessels, and valvular regurgitation.
Implanted metallic devices (eg, coils, stents, pacemakers) may cause imaging artifact or may require modification of MRI protocol; in some cases, they may preclude MRI altogether. (See also Magnetic Resonance Imaging of the Chest.)

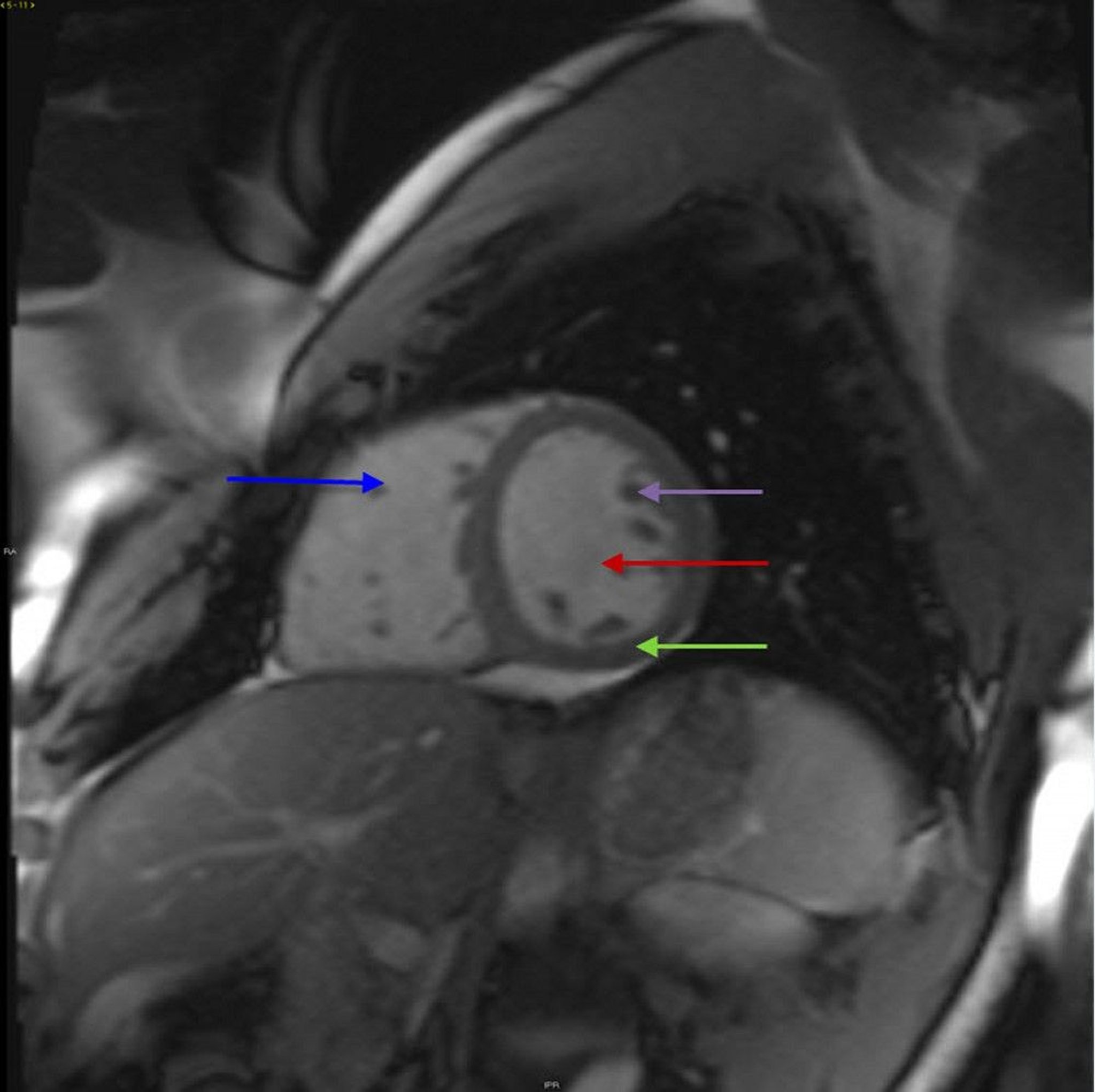
This image shows a normal left ventricle (red arrow), right ventricle (blue arrow), and myocardium (green arrow). Papillary muscles (purple arrow) are also visible.
© 2017 Elliot K. Fishman, MD.
Sequential MRI (contrast MRI) after injection of a paramagnetic contrast agent (gadolinium-diethylenetriamine pentaacetic acid [Gd-DTPA]) produces higher resolution of myocardial perfusion patterns than does radionuclide imaging. MRI is generally considered the most accurate and reliable measure of ventricular volumes as well as ejection fraction. However, patients with impaired renal function (those with glomerular filtration rate < 30 mL/minute, or receiving renal replacement therapy) can develop nephrogenic systemic fibrosis, a potentially life-threatening disorder, after use of gadolinium contrast.
When MRI is performed with contrast, 3-dimensional information on infarct size and location can be obtained, and blood flow velocities in cardiac chambers can be measured. MRI can assess tissue viability by assessing the contractile response to inotropic stimulation with dobutamine, or by using gadolinium contrast (which is excluded from cells with intact membranes, resulting in delayed or late gadolinium enhancement of fibrotic areas). MRI discriminates myocardial scar from inflammation with edema and is helpful in diagnosing myocarditis. In patients with Marfan syndrome, MRI measurements of ascending aorta dilation are more accurate than echocardiographic measurements. MRI is used regularly in the evaluation of nonischemic cardiomyopathies such as amyloidosis. MRI is also important in evaluating complex congenital heart disease from both an anatomic and a functional standpoint.
Magnetic resonance angiography (MRA), after injection of a gadolinium contrast agent, is used to assess blood volumes of interest (eg, blood vessels in the chest or abdomen); all blood flow can be assessed simultaneously. MRA can be used to detect aneurysms, stenosis, or occlusions in the carotid, coronary, renal, or peripheral arteries.
Magnetic resonance venography (MRV) can be used as an alternative to ultrasound to detect deep venous thrombosis; however, MRV is less well established and more expensive than ultrasound.
Cardiac MR is also used in stress testing.
Radionuclide Imaging
Single positron emission CT (SPECT) and positron emission tomography (PET) are radionuclide imaging modes used in cardiac imaging. They rely on the detection of radionuclides to identify sites of uptake, indicating perfusion, metabolic activity, nonviable tissue, or infiltration. Both are used in assessing for coronary artery disease, with SPECT being more widely available and less expensive, and PET providing superior image quality and accuracy at higher cost (1). Other indications for radionuclide imaging include valvular function, ventriculography, and evaluating for inflammatory and infiltrative disease.
Radionuclide imaging reference
1. Knott JD, Kronzer E, Anavekar N, Chareonthaitawee P, Askew JW. Radionuclide imaging techniques for assessing myocardial viability: Clinical applications, evidence, and future directions. Prog Cardiovasc Dis. 2025;93:51-59. doi:10.1016/j.pcad.2025.08.005
Drug Information for the Topic





