

Almost all patients with deep venous thrombosis (DVT) are given anticoagulants and in < 5% of cases thrombolytics. A number of anticoagulants are effective for management of deep venous thrombosis (see also Treatment of Deep Venous Thrombosis).
Anticoagulants
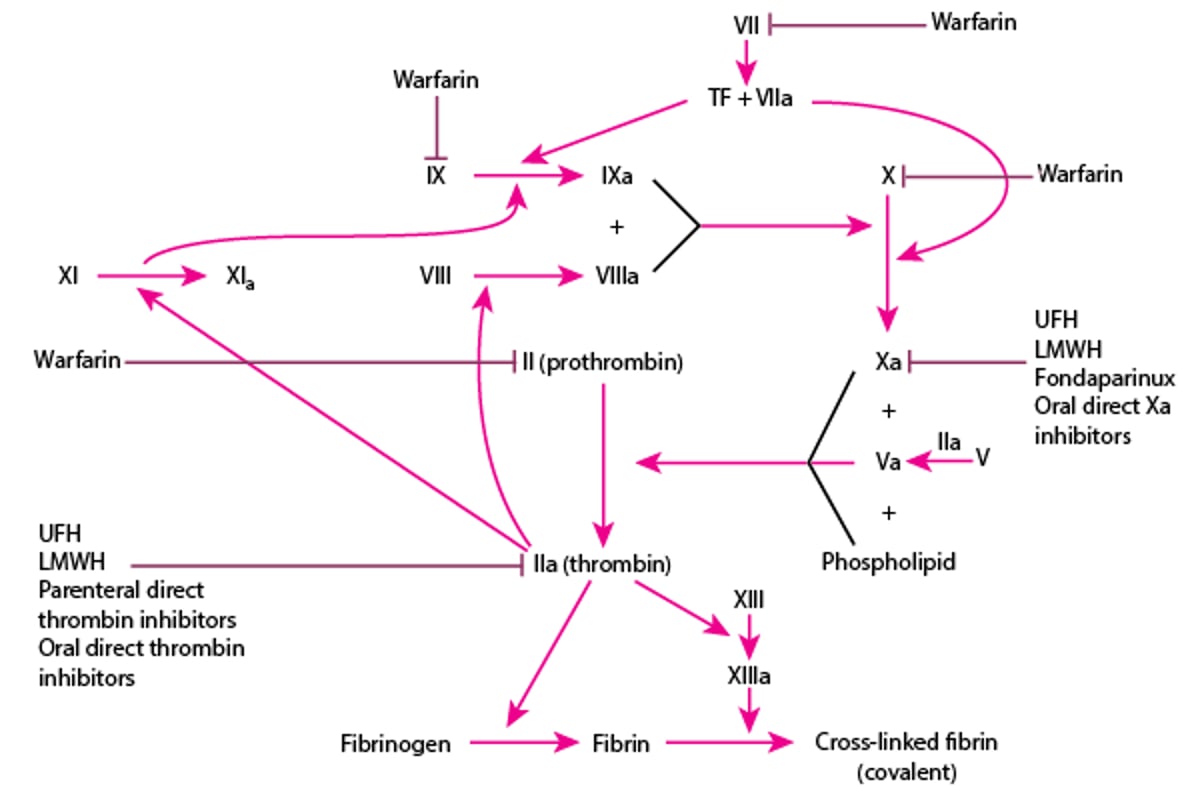
The anticoagulants (see figure and table ) include:
Low molecular weight heparins (LMWHs)
Unfractionated heparin (UFH)Unfractionated heparin (UFH)
Factor Xa inhibitors: oral (eg, rivaroxaban, apixaban, edoxaban) and parenteral (fondaparinux)inhibitors: oral (eg, rivaroxaban, apixaban, edoxaban) and parenteral (fondaparinux)
Direct thrombin inhibitors: oral (dabigatran etexilate) and parenteral (argatroban, bivalirudin, desirudin)inhibitors: oral (dabigatran etexilate) and parenteral (argatroban, bivalirudin, desirudin)
WarfarinWarfarin
Oral factor Xa inhibitors and direct thrombin inhibitors are sometimes referred to as direct oral anticoagulants (DOACs). However, there are also parenteral agents that inhibit both factor Xa and thrombin (unfractionated heparin), that inhibit mainly (unfractionated heparin), that inhibit mainlyfactor Xa (LMWH), or that inhibit only factor Xa (fondaparinux). These agents can be used both for patients with DVT and those with pulmonary embolism (PE). (fondaparinux). These agents can be used both for patients with DVT and those with pulmonary embolism (PE).
See Treatment of Deep Venous Thrombosis for a discussion of anticoagulation strategies including selection, initiation, and duration of therapy.
Anticoagulants and Their Sites of Action
LMWH = low molecular weight heparin; TF = tissue factor; UFH = unfractionated heparin. |

Direct Oral Anticoagulants for Treatment of Venous Thromboembolism
Medication | Dose | Comments |
|---|---|---|
Factor Xa inhibitors | ||
ApixabanApixaban | 10 mg twice a day for 7 days Then 5 mg twice a day | Apixaban should not be used for DVT or PE if creatinine clearance is Apixaban should not be used for DVT or PE if creatinine clearance is< 30 mL/minute (0.5mL/s/m2). Dosage may be lowered to 2.5 mg twice a day after 6–12 months of treatment. |
EdoxabanEdoxaban | 60 mg once a day If creatinine clearance is 15–50 mL/minute (0.25 to 0.83 mL/s/m2) or if body weight is ≤ 60 kg, 30 mg once a day | Initial treatment with a low molecular weight heparin is needed for 5 days.Initial treatment with a low molecular weight heparin is needed for 5 days. Edoxaban should not be used if creatinine clearance is Edoxaban should not be used if creatinine clearance is< 15 mL/minute (0.25 mL/s/m2). |
RivaroxabanRivaroxaban | 15 mg twice a day for 21 days taken with food Then 20 mg once a day taken with food | Rivaroxaban should not be used for DVT or PE if creatinine clearance is Rivaroxaban should not be used for DVT or PE if creatinine clearance is< 30 mL/minute (0.5mL/s/m2). Dosage may be lowered to 10 mg once a day after 6–12 months of treatment. |
Factor IIa (thrombin) inhibitor | ||
DabigatranDabigatran | 150 mg twice a day | Initial treatment with low molecular weight heparin is needed for 5 days.Initial treatment with low molecular weight heparin is needed for 5 days. Dabigatran should not be used for DVT if creatinine clearance is Dabigatran should not be used for DVT if creatinine clearance is< 30 mL/minute (0.5mL/s/m2). |
DVT = deep venous thrombosis; PE = pulmonary embolism. | ||
Factor Xa inhibitors
Rivaroxaban and apixaban can be started as monotherapy immediately upon diagnosis or used in transition from an injectable heparin at any time without overlap (Rivaroxaban and apixaban can be started as monotherapy immediately upon diagnosis or used in transition from an injectable heparin at any time without overlap (1). Dosing of rivaroxaban is 15 mg orally twice a day for 3 weeks followed by 20 mg orally once a day for a total of 3 to 6 months. Apixaban dosing is 10 mg orally twice a day for 7 days followed by 5 mg orally twice a day for 3 to 6 months.
Before edoxaban is started, an initial 5 to 7 days of treatment with LMWH or UFH is required. Then edoxaban is given 60 mg orally once a day. To transition from an injectable anticoagulant, the Before edoxaban is started, an initial 5 to 7 days of treatment with LMWH or UFH is required. Then edoxaban is given 60 mg orally once a day. To transition from an injectable anticoagulant, thefactor Xa inhibitor is typically started within 6 to 12 hours after the last dose of a twice-daily LMWH regimen and within 12 to 24 hours after a once-daily LMWH regimen.
There is evidence that apixaban, edoxaban, and rivaroxaban can be used in select patients with cancer-associated venous thromboembolism (VTE) as an alternative to monotherapy with LMWH (There is evidence that apixaban, edoxaban, and rivaroxaban can be used in select patients with cancer-associated venous thromboembolism (VTE) as an alternative to monotherapy with LMWH (2, 3, 4, 5).
Fondaparinux, a parenteral selective Fondaparinux, a parenteral selectivefactor Xa inhibitor, may be used as an alternative to UFH or LMWH for the initial treatment of DVT or PE. It is given in a fixed dose of 7.5 mg subcutaneously once a day (10 mg for patients > 100 kg, 5 mg for patients < 50 kg). It has the advantage of fixed dosing and is less likely to cause thrombocytopenia.
Direct thrombin inhibitors
Dabigatran 150 mg orally twice a day is given only after an initial 5 days of treatment with LMWH (Dabigatran 150 mg orally twice a day is given only after an initial 5 days of treatment with LMWH (1). It is typically started within 6 to 12 hours after the last dose of a twice-daily LMWH regimen and within 12 to 24 hours after a once-daily regimen.
Parenteral direct thrombin inhibitors (argatroban, bivalirudin, desirudin) are available but do not have a role in treatment or inhibitors (argatroban, bivalirudin, desirudin) are available but do not have a role in treatment orprevention of DVT or PE. Argatroban may be useful to treat DVT in patients with of DVT or PE. Argatroban may be useful to treat DVT in patients withheparin-induced thrombocytopenia (6).
Vitamin K antagonists (warfarin)
Warfarin is a treatment option for patients with DVT who are not pregnant. It is also an option for patients with severe renal dysfunction. Warfarin is a treatment option for patients with DVT who are not pregnant. It is also an option for patients with severe renal dysfunction.Warfarin is also a second-line option for patients with cancer-associated VTE.
Warfarin can be started, initially at a dose of 5 to 10 mg once daily, immediately along with heparin because it takes about 5 days to achieve desired therapeutic effect. Older patients and patients with a liver disorder typically require lower can be started, initially at a dose of 5 to 10 mg once daily, immediately along with heparin because it takes about 5 days to achieve desired therapeutic effect. Older patients and patients with a liver disorder typically require lowerwarfarin doses. Therapeutic goal is an international normalized ratio (INR) of 2.0 to 3.0 (1). INR is monitored weekly for the first 1 to 2 months of warfarin treatment and monthly thereafter; the dose is adjusted to maintain the INR within this range. Patients taking warfarin should be informed of possible medication interactions, including interactions with foods and nonprescription medicinal herbs.
Rarely, warfarin causes skin necrosis in patients with inherited protein C deficiency or protein S deficiency.
Low molecular weight heparins (LMWHs)
A low molecular weight heparin (LMWH, eg, enoxaparin, dalteparin, tinzaparin)can be given on an outpatient basis. Like UFH, LMWHs catalyze the action of antithrombin (which inhibits coagulation factor proteases), leading to inactivation of coagulation (LMWH, eg, enoxaparin, dalteparin, tinzaparin)can be given on an outpatient basis. Like UFH, LMWHs catalyze the action of antithrombin (which inhibits coagulation factor proteases), leading to inactivation of coagulationfactor Xa and, to a lesser degree, factor IIa. LMWHs also have some antithrombin–mediated anti-inflammatory properties, which facilitate clot organization and resolution of symptoms and inflammation. LMWHs are as effective as unfractionated heparin (UFH) for reducing DVT recurrence, thrombus extension, and risk of death due to PE (7). The primary indications for LMWH as a first-line therapy are for DVT in pregnant patients and for breakthrough DVT in patients taking warfarin, in which case it is preferred over DOACs (). The primary indications for LMWH as a first-line therapy are for DVT in pregnant patients and for breakthrough DVT in patients taking warfarin, in which case it is preferred over DOACs (1, 8, 9).
LMWHs are typically given subcutaneously in a standard weight-based dose (eg, enoxaparin 1.5 mg/kg subcutaneously once a day or 1 mg/kg subcutaneously every 12 hours or dalteparin 200 units/kg subcutaneously once a day). Patients with renal insufficiency may be treated with UFH or with reduced doses of LMWH. Monitoring is not reliable because LMWHs do not significantly prolong the results of global tests of coagulation. Furthermore, they have a predictable dose response, and there is no clear relationship between the anticoagulant effect of LMWH and bleeding. If warfarin is used after initial anticoagulation, treatment with LMWH is continued until full anticoagulation is achieved with LMWHs are typically given subcutaneously in a standard weight-based dose (eg, enoxaparin 1.5 mg/kg subcutaneously once a day or 1 mg/kg subcutaneously every 12 hours or dalteparin 200 units/kg subcutaneously once a day). Patients with renal insufficiency may be treated with UFH or with reduced doses of LMWH. Monitoring is not reliable because LMWHs do not significantly prolong the results of global tests of coagulation. Furthermore, they have a predictable dose response, and there is no clear relationship between the anticoagulant effect of LMWH and bleeding. If warfarin is used after initial anticoagulation, treatment with LMWH is continued until full anticoagulation is achieved withwarfarin (typically about 5 days). Transition to the oral agents rivaroxaban or apixaban can be done at any time with no overlap. Transition to edoxaban or dabigatran requires at least 5 days of LMWH treatment, but no overlap is needed.(typically about 5 days). Transition to the oral agents rivaroxaban or apixaban can be done at any time with no overlap. Transition to edoxaban or dabigatran requires at least 5 days of LMWH treatment, but no overlap is needed.
Complications of LMWHs include bleeding, thrombocytopenia, urticaria, and, rarely, thrombosis and anaphylaxis. Inpatients and possibly outpatients should be screened for bleeding with serial complete blood counts and, where appropriate, testing for occult blood in stool.
Unfractionated heparin (UFH)
Unfractionated heparin may be used instead of LMWH for patients who are hospitalized and for patients who have chronic kidney disease with a creatinine clearance 10 to 30 mL/minute, (0.17 to 0.5mL/s/mUnfractionated heparin may be used instead of LMWH for patients who are hospitalized and for patients who have chronic kidney disease with a creatinine clearance 10 to 30 mL/minute, (0.17 to 0.5mL/s/m2) because UFH is not cleared by the kidneys. UFH is given as a bolus and infusion to achieve full anticoagulation (eg, activated partial thromboplastin time [aPTT] 1.5 to 2.5 times that of the reference range). For outpatients, UFH 333 units/kg initial bolus, then 250 units/kg subcutaneously every 12 hours can be substituted for IV UFH to facilitate mobility; the dose does not need adjustment based on aPTT. If warfarin is used after initial anticoagulation, UFH is continued until full anticoagulation has been achieved with ) because UFH is not cleared by the kidneys. UFH is given as a bolus and infusion to achieve full anticoagulation (eg, activated partial thromboplastin time [aPTT] 1.5 to 2.5 times that of the reference range). For outpatients, UFH 333 units/kg initial bolus, then 250 units/kg subcutaneously every 12 hours can be substituted for IV UFH to facilitate mobility; the dose does not need adjustment based on aPTT. If warfarin is used after initial anticoagulation, UFH is continued until full anticoagulation has been achieved withwarfarin (usually about 5 days).
Complications of UFH are similar to those of LMWHs, except that heparin-induced thrombocytopenia, which is rare and may be life-threatening, is more common with UFHs. Long-term use of UFH causes hyperkalemia, liver enzyme elevations, and osteopenia. Rarely, UFH given subcutaneously causes skin necrosis. Inpatients and possibly outpatients being given UFH should be screened for bleeding.
Bleeding During Use of Anticoagulants
Bleeding is the most common complication of anticoagulants and ranges on a continuum from minor to severe, life-threatening hemorrhage.
For minor bleeding (eg, epistaxis), local measures to stop bleeding (eg, direct pressure) are often sufficient. The anticoagulant is usually not discontinued or reversed unless bleeding becomes more severe.
For severe bleeding (eg, heavy gastrointestinal bleeding), the anticoagulant is usually discontinued (at least temporarily) and other measures taken. Bleeding is generally considered severe when it is:
Heavy (loss of ≥ 2 units of blood in ≤ 7 days)
In a critical location (eg, intracranial, intraocular)
In a location where hemostasis is difficult to achieve (eg, small bowel, posterior nasal cavity, lung)
Risk factors for severe bleeding include (1, 2):
Age ≥ 65 to 75 years
History of prior gastrointestinal bleeding or stroke
Recent myocardial infarction
Coexisting anemia (hematocrit < 30%), end-stage renal disease (serum creatinine > 1.5 mg/dL [115 micromol/L]), or diabetes
Thrombocytopenia
Active cancer
Supportive care for severe bleeding includes local measures to stop bleeding (eg, direct pressure, cauterization, injection). Patients with signs and symptoms of volume loss and those with heavy ongoing bleeding may require intravenous fluid resuscitation and packed red blood cell transfusions. These measures are sufficient for many bleeding episodes.
In patients with life-threatening and/or ongoing bleeding or bleeding in a critical location, clinicians also consider giving:
Reversal agents
Clotting factors (eg, prothrombin complex concentrate, fresh frozen plasma)Clotting factors (eg, prothrombin complex concentrate, fresh frozen plasma)
Antifibrinolytics
However, by definition these agents are prothrombotic, and the risks of continued bleeding should be balanced with the increased risk of thrombosis.
Anticoagulant reversal
Many of the anticoagulants have specific reversal agents. If these are unavailable or ineffective, clotting factors, typically in the form of 4-factor prothrombin complex concentrate or sometimes fresh frozen plasma, can be given. Some anticoagulants can be removed by hemodialysis or have absorption blocked by activated charcoal.Many of the anticoagulants have specific reversal agents. If these are unavailable or ineffective, clotting factors, typically in the form of 4-factor prothrombin complex concentrate or sometimes fresh frozen plasma, can be given. Some anticoagulants can be removed by hemodialysis or have absorption blocked by activated charcoal.
With the heparins, bleeding can be stopped or slowed with protamine (bleeding can be stopped or slowed with protamine (3). It is more effective on unfractionated heparin (UFH) than on low molecular weight heparin (LMWH) because ). It is more effective on unfractionated heparin (UFH) than on low molecular weight heparin (LMWH) becauseprotamine only partially neutralizes LMWH inactivation of factor Xa. During all infusions, patients should be observed for hypotension and a reaction similar to an anaphylactic reaction. Because UFH given IV has a half-life of 30 to 60 minutes, protamine is typically not given to patients who have received UFH > 60 to 120 minutes beforehand) or is given at a reduced dose based on the amount of heparin estimated to be remaining in plasma, based on the half-life of UFH.
WarfarinWarfarin anticoagulation can be reversed with vitamin K (3). If hemorrhage is severe, prothrombin complex concentrate should be given; fresh frozen plasma may be used if ). If hemorrhage is severe, prothrombin complex concentrate should be given; fresh frozen plasma may be used ifprothrombin complex concentrate is unavailable. Selected patients with overanticoagulation (INR 5 to 9) who are neither actively bleeding nor at increased risk of bleeding can be managed by omitting 1 or 2 warfarin doses and monitoring INR more frequently, then giving warfarin at a lower dose.
With dabigatran,dabigatran, a humanized monoclonal antibody idarucizumab is an effective antidote to bleeding (a humanized monoclonal antibody idarucizumab is an effective antidote to bleeding (3). If the agent is not available, 4-factor prothrombin complex concentratecan be given. Hemodialysis also may help because dabigatran is not highly protein bound. Oral activated charcoal is an option if the last dose of is not highly protein bound. Oral activated charcoal is an option if the last dose ofdabigatran was within 2 hours.
With factor Xa inhibitors, andexanet alfa is an antidote available in the United States; however, its use is restricted in part due to its high cost (3, 4). Fondaparinux anticoagulation can theoretically also be reversed with ). Fondaparinux anticoagulation can theoretically also be reversed withandexanet alfa although this has not been studied in research trials. If andexanet alfa is unavailable, 4-factor prothrombin complex concentrate may be considered. Oral activated charcoal is an option in patients who took an oral may be considered. Oral activated charcoal is an option in patients who took an oralfactor Xa inhibitor within a few hours of presentation (8 hours for rivaroxaban, 6 hours for apixaban, and 2 hours for edoxaban). Hemodialysis is not effective for removal of the oral factor Xa inhibitors.
Clotting factors
Clotting factors are available in the form of:
Prothrombin complex concentrateProthrombin complex concentrate
Fresh frozen plasma
Individual clotting factors
Prothrombin complex concentrate is available in several forms. Three-factor prothrombin complex concentrate contains high levels of factors II, IX, and X, and 4-factor prothrombin complex concentrate adds factor VII; both also contain protein C and protein S. Prothrombin complex concentrate can be unactivated or activated, in which some of the factors have been cleaved to their active forms. Four-factor prothrombin complex concentrate is preferred as it tends to be more effective at reversing bleeding than the 3-factor form (3, 5). If 3-factor prothrombin complex concentrate is used, fresh frozen plasma can also be given because fresh frozen plasma contains factor VII. Typical dose is 50 units/kg IV. Because evidence of benefit is uncertain and risk of clotting is significant, prothrombin complex concentrates should be reserved for life-threatening bleeding.
Fresh frozen plasma contains all the clotting factors but only at normal plasma levels. It is typically used only if prothrombin complex concentrate is unavailable; there is no evidence it is effective in bleeding due to Fresh frozen plasma contains all the clotting factors but only at normal plasma levels. It is typically used only if prothrombin complex concentrate is unavailable; there is no evidence it is effective in bleeding due tofactor Xa inhibitors (3).
Individual clotting factors such as activated recombinant factor VII are available but are not thought to be helpful for anticoagulant-related bleeding.
Antifibrinolytics and other agents
Antifibrinolytic agents (tranexamic acid and aminocaproic acid) can also be tried; however, their use has not been studied for reversal of bleeding in patients taking anticoagulants.Antifibrinolytic agents (tranexamic acid and aminocaproic acid) can also be tried; however, their use has not been studied for reversal of bleeding in patients taking anticoagulants.
Resumption of anticoagulation after bleeding
Clinical judgment is necessary when deciding whether to permanently stop or lower the dose of anticoagulant.
If a patient has almost completed their treatment course of anticoagulant and has a severe bleeding episode, the anticoagulant can be stopped. However, if a patient has just started or is mid-way through their treatment course and has a severe bleed, the decision of whether to stop or reduce the dose of anticoagulant is not as straightforward and should be made in consultation with a multidisciplinary team and keeping in mind the patient's priorities.
Bleeding due to anticoagulants references
1. Ageno W, Gallus AS, Wittkowsky A, Crowther M, Hylek EM, Palareti G. Oral anticoagulant therapy: Antithrombotic Therapy and Prevention of Thrombosis, 9th ed: American College of Chest Physicians Evidence-Based Clinical Practice Guidelines. Chest. 2012;141(2 Suppl):e44S-e88S. doi:10.1378/chest.11-2292
2. Kim K, Yamashita Y, Morimoto T, et al. Risk Factors for Major Bleeding during Prolonged Anticoagulation Therapy in Patients with Venous Thromboembolism: From the COMMAND VTE Registry. Thromb Haemost. 2019;119(9):1498-1507. doi:10.1055/s-0039-1692425
3. Tomaselli GF, Mahaffey KW, Cuker A, et al. 2020 ACC Expert Consensus Decision Pathway on Management of Bleeding in Patients on Oral Anticoagulants: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2020;76(5):594-622. doi:10.1016/j.jacc.2020.04.053
4. Connolly SJ, Crowther M, Eikelboom JW, et al. Full study report of andexanet alfa for bleeding associated with factor Xa inhibitors. N Engl J Med. 2019;380:1326-1335. doi: 10.1056/NEJMoa1814051
5. Puchstein D, Kork F, Schöchl H, Rayatdoost F, Grottke O. 3-Factor versus 4-Factor Prothrombin Complex Concentrates for the Reversal of Vitamin K Antagonist-Associated Coagulopathy: A Systematic Review and Meta-analysis. Thromb Haemost. 2023;123(1):40-53. doi:10.1055/s-0042-1758653
Thrombolytic (Fibrinolytic) Agents
Thrombolytic agents, which include alteplase, tenecteplase, and streptokinase, lyse clots and may be more effective than heparin alone in selected patients with DVT, but the risk of bleeding is higher than with Thrombolytic agents, which include alteplase, tenecteplase, and streptokinase, lyse clots and may be more effective than heparin alone in selected patients with DVT, but the risk of bleeding is higher than withheparin alone. For patients with DVT, a clinical trial showed that catheter-directed thrombolytic therapy did not reduce the incidence of post-thrombotic syndrome compared with conventional anticoagulant therapy (1). However, thrombolytic agents can be considered only in highly selected patients with DVT (2). Patients who may benefit from thrombolytic agents include those with extensive iliofemoral DVT who are younger (< 60 years) and do not have risk factors for bleeding. Thrombolytic therapy should be given stronger consideration in patients with extensive DVT who have evolving or existing limb ischemia (eg, phlegmasia cerulea dolens).
Catheter-directed thrombolysis is preferred over systemic thrombolysis for patients with extensive DVT in whom thrombolysis is used (3).
Bleeding, if it occurs, is most often at the site of arterial or venous puncture sites. This complication can be treated by stopping the thrombolytic agent and doing mechanical compression or surgical repair of the puncture site. Life-threatening bleeding is treated with cryoprecipitate and fresh frozen plasma in addition to stopping the thrombolytic agent.
Thrombolytic treatment references
1. Vedantham S, Goldhaber SZ, Julien JA, et al. Pharmacomechanical catheter-directed thrombolysis for deep-vein thrombosis. N Engl J Med. 2017;377:2240–2252. doi: 10.1056/NEJMoa1615066
2. Kahn SR, Comerota AJ, Cushman M, et al. The postthrombotic syndrome: evidence-based prevention, diagnosis, and treatment strategies: a scientific statement from the American Heart Association. Circulation. 2014;130(18):1636-1661. doi:10.1161/CIR.0000000000000130
3. Ortel TL, Neumann I, Ageno W, et al. American Society of Hematology 2020 guidelines for management of venous thromboembolism: treatment of deep vein thrombosis and pulmonary embolism. Blood Adv. 2020;4(19):4693-4738. doi:10.1182/bloodadvances.2020001830
Drug Information for the Topic





