



Vitiligo is a loss of skin melanocytes that causes areas of skin depigmentation of varying sizes. Cause is unknown, but genetic and autoimmune factors are likely. Diagnosis is usually clear based on skin examination. Common treatments include topical corticosteroids (often combined with calcipotriene), calcineurin inhibitors (tacrolimus and pimecrolimus), and narrowband ultraviolet (UV) B. For widespread disease, narrowband UVB is often the treatment of choice. For severe widespread pigment loss, residual patches of normal skin may be permanently depigmented (bleached) with monobenzyl ether of hydroquinone. Surgical skin grafting and tattooing may also be considered.
(See also Overview of Pigmentation Disorders.)
Vitiligo affects up to 2% of the population (1).
Reference
1. Krüger C, Schallreuter KU. A review of the worldwide prevalence of vitiligo in children/adolescents and adults. Int J Dermatol. 2012;51(10):1206-1212. doi:10.1111/j.1365-4632.2011.05377.x
Etiology of Vitiligo
Etiology of vitiligo is unclear, but melanocytes are lacking in affected areas. Proposed mechanisms include autoimmune destruction of melanocytes, reduced survival of melanocytes, and primary melanocyte defects.
Vitiligo can be familial (autosomal dominant with incomplete penetrance and variable expression) or acquired. Some patients have antibodies to melanin. Up to 30% of patients have other autoimmune antibodies (to thyroglobulin, adrenal cells, and parietal cells) or clinical autoimmune endocrinopathies (eg, Addison disease, diabetes mellitus, pernicious anemia, thyroid dysfunction) (1, 2). However, the relationship is unclear and may be coincidental. The strongest association is with Graves disease and Hashimoto thyroiditis.
Occasionally, vitiligo occurs after a direct physical injury to the skin (eg, as a response to sunburn). Vitiligo can also result from exposure to certain chemicals found in household products and dyes (3). Patients may associate the onset of vitiligo with emotional stress.
Immunotherapy for melanoma (eg, BRAF inhibitors, programmed death receptor 1 [PD-1] inhibitors) can trigger vitiligo as an immunologic adverse effect (4).
Etiology references
1. Sheth VM, Guo Y, Qureshi AA. Comorbidities associated with vitiligo: a ten-year retrospective study. Dermatology. 2013;227(4):311-315. doi:10.1159/000354607
2. Rios-Duarte JA, Sanchez-Zapata MJ, Silverberg JI. Association of vitiligo with multiple cutaneous and extra-cutaneous autoimmune diseases: a nationwide cross-sectional study. Arch Dermatol Res. 2023;315(9):2597-2603. doi:10.1007/s00403-023-02661-y
3. Harris JE. Chemical-Induced Vitiligo. Dermatol Clin. 2017;35(2):151-161. doi:10.1016/j.det.2016.11.006
4. Burzi L, Alessandrini AM, Quaglino P, Piraccini BM, Dika E, Ribero S. Cutaneous Events Associated with Immunotherapy of Melanoma: A Review. J Clin Med. 2021;10(14):3047. Published 2021 Jul 8. doi:10.3390/jcm10143047
Symptoms and Signs of Vitiligo
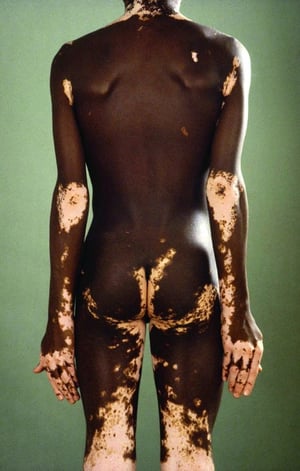
Vitiligo is characterized by hypopigmented or depigmented areas, usually sharply demarcated and often symmetric. Depigmentation may be localized, involving 1 or 2 spots or entire body segments (segmental vitiligo); rarely, it may be generalized, involving most of the skin surface (universal vitiligo). However, vitiligo most commonly involves the face (especially around the orifices), digits, dorsal hands, flexor wrists, elbows, knees, shins, dorsal ankles, armpits, inguinal area, anogenital area, umbilicus, and nipples. Cosmetic disfigurement can be especially severe and emotionally devastating in patients with dark skin. Hair in vitiliginous areas is usually white.


This photo shows focal vitiligo of the foot.
This photo shows focal vitiligo of the foot.
Photo provided by Thomas Habif, MD.


© Springer Science+Business Media


Photo courtesy of Karen McKoy, MD.


The cosmetic disfigurement shown in this photo is significant.
The cosmetic disfigurement shown in this photo is significant.
© Springer Science+Business Media


Photo courtesy of Karen McKoy, MD.


© Springer Science+Business Media


© Springer Science+Business Media


© Springer Science+Business Media

© Springer Science+Business Media
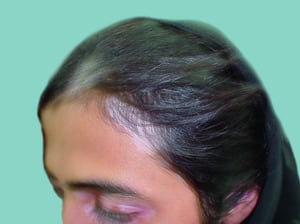
Hair in vitiliginous areas is usually white.
Hair in vitiliginous areas is usually white.
© Springer Science+Business Media


Photo courtesy of Karen McKoy, MD.
This photo shows focal vitiligo of the foot.
This photo shows focal vitiligo of the foot.
Photo provided by Thomas Habif, MD.
© Springer Science+Business Media
Photo courtesy of Karen McKoy, MD.
The cosmetic disfigurement shown in this photo is significant.
The cosmetic disfigurement shown in this photo is significant.
© Springer Science+Business Media
Photo courtesy of Karen McKoy, MD.
© Springer Science+Business Media
© Springer Science+Business Media
© Springer Science+Business Media
© Springer Science+Business Media
Hair in vitiliginous areas is usually white.
Hair in vitiliginous areas is usually white.
© Springer Science+Business Media
Photo courtesy of Karen McKoy, MD.
Diagnosis of Vitiligo
Clinical evaluation
Depigmented skin is typically obvious on examination, especially in people with dark skin.
Subtle hypopigmented or depigmented lesions are accentuated under a Wood light (365 nm), which shows the chalk-white appearance of depigmented skin.


Vitiligo is accentuated under a Wood light (right).
Differential diagnosis includes postinflammatory hypopigmentation, piebaldism (a rare autosomal dominant disorder in which depigmented patches surrounded by hyperpigmented areas occur most often on the forehead, neck, anterior trunk, and mid-extremities), morphea (localized scleroderma, in which skin is usually sclerotic), leprosy (in which lesions are usually hypoesthetic), lichen sclerosus, pityriasis alba, chemical leukoderma, and leukoderma due to melanoma.
Although there are no evidence-based guidelines, it is reasonable for physicians to test with complete blood count, fasting blood glucose, thyroid function, and antithyroid peroxidase antibodies (frequently present in Hashimoto thyroiditis) as clinically indicated by review of systems.
Treatment of Vitiligo
Protection of affected areas from sunlight
Topical corticosteroids and calcipotriene
Topical calcineurin inhibitors for face or groin involvement
Narrowband ultraviolet B (UVB)
Vitiligo can be challenging to manage; initial repigmentation and maintenance of pigment can be unpredictable. Physicians must be aware of individual and ethnic sensibilities regarding uniform skin coloring; the disease can be psychologically devastating. All depigmented areas are prone to severe sunburn and must be protected with clothing or sunscreen.
Small, scattered lesions may be camouflaged with makeup. With more extensive involvement, treatment is usually aimed at repigmentation. Although little is known about comparative efficacies of many such treatments, reviews (1) and consensus recommendations (2) have been recently published. Traditional first-line therapy is potent topical corticosteroids, which may also cause hypopigmentation or atrophy in normal surrounding skin as an adverse effect of chronic corticosteroid use. Calcineurin inhibitors (tacrolimus and pimecrolimus) may be particularly useful alternatives for treating areas of the skin, such as the face and groin, where adverse effects of topical corticosteroid therapy most commonly occur. Calcipotriene blended with betamethasone dipropionate may also be helpful and more successful than monotherapy with either medication.
Narrowband UVB (NB-UVB) is often the preferred initial treatment for widespread vitiligo, especially in patients for whom immunosuppression is contraindicated (3). Excimer (308 nm) laser may be useful, particularly for patients with localized disease that does not respond to initial topical therapy. When considering phototherapy, the theoretical increased risk of skin cancers should be discussed with patients. Patients undergoing phototherapy may benefit from regular skin cancer screenings.
In patients with rapidly progressing vitiligo (over weeks to months), a low-dose oral corticosteroid for a couple of weeks can be considered to limit the spread. Because oral corticosteroids do not repigment the skin, NB-UVB can be added to facilitate repigmentation.
Surgery is reasonable only for patients with stable, limited disease when medical therapy has failed. Therapies include autologous micrografting (4), suction blister grafting, and tattooing; tattooing is especially useful for difficult-to-repigment areas such as the nipples, lips, and fingertips.
Depigmentation of unaffected skin to achieve homogeneous skin tone is possible with 20% monobenzyl ether of hydroquinone applied twice a day. This treatment is indicated only when most of the skin is involved and the patient is prepared for permanent pigment loss and the subsequent increased risks of photo-induced skin damage (eg, skin cancers, photoaging). This treatment can be extremely irritating, so a smaller test area should be treated before widespread use. Treatment for ≥ 1 year may be required.
The topical Janus kinase (JAK) inhibitor ruxolitinib (JAK 1 and 2) is available for the treatment of vitiligo (5). Another JAK inhibitor, tofacitinib (JAK 1 and 3), is currently under investigation. However, depigmentation can recur after these agents are stopped.
Treatment references
1. Kubelis-López DE, Zapata-Salazar NA, Said-Fernández SL, et al. Updates and new medical treatments for vitiligo (Review). Exp Ther Med. 2021;22(2):797. doi:10.3892/etm.2021.10229
2. van Geel N, Speeckaert R, Taïeb A, et al. Worldwide expert recommendations for the diagnosis and management of vitiligo: Position statement from the International Vitiligo Task Force Part 1: towards a new management algorithm. J Eur Acad Dermatol Venereol. 2023;37(11):2173-2184. doi:10.1111/jdv.19451
3. Esmat SM, El-Mofty M, Rasheed H, et al. Efficacy of narrow band UVB with or without OMP in stabilization of vitiligo activity in skin photo-types (III-V): A double-blind, randomized, placebo-controlled, prospective, multicenter study. Photodermatol Photoimmunol Photomed. 2022;38(3):277-287. doi:10.1111/phpp.12749
4. Gan EY, Kong YL, Tan WD, et al. Twelve-month and sixty-month outcomes of noncultured cellular grafting for vitiligo. J Am Acad Dermatol. 2016;75(3):564-571. doi:10.1016/j.jaad.2016.04.007
5. Phan K, Phan S, Shumack S, Gupta M. Repigmentation in vitiligo using janus kinase (JAK) inhibitors with phototherapy: systematic review and Meta-analysis. J Dermatolog Treat. 2022;33(1):173-177. doi:10.1080/09546634.2020.1735615.
Key Points
Some cases of vitiligo may involve genetic mutations or autoimmune disorders.
Vitiligo can be focal, segmental, or, rarely, generalized.
Diagnose by skin examination, but consider testing with complete blood count, fasting blood glucose, thyroid function tests, and antithyroid peroxidase antibodies.
Consider treatments such as topical calcipotriene plus betamethasone dipropionate, corticosteroid topical monotherapy, narrowband UVB, or a calcineurin inhibitor (tacrolimus and pimecrolimus).
Janus kinase inhibitors are an emerging treatment modality for vitiligo.
Drug Information for the Topic





