



Hypokalemia is serum potassium concentration < 3.5 mEq/L (< 3.5 mmol/L) caused by a deficit in total body potassium stores or abnormal movement of potassium into cells. The most common cause is excess loss from the kidneys or gastrointestinal tract. Intracellular shifts as well as certain medications can also cause hypokalemia. Clinical features include muscle weakness and polyuria; cardiac hyperexcitability may occur with severe hypokalemia. Diagnosis is by serum measurement. Treatment is giving potassium and managing the cause.
(See also Overview of Disorders of Potassium Concentration.)
Etiology of Hypokalemia
Hypokalemia can be caused by decreased intake of potassium but is usually caused by excessive losses of potassium in the urine or from the gastrointestinal (GI) tract.
Gastrointestinal tract losses
Abnormal GI potassium losses occur in all of the following:
Chronic diarrhea, including chronic laxative abuse and bowel diversion
Clay (bentonite) ingestion, which binds potassium and greatly decreases absorption
Rarely, villous adenoma of the colon, which causes massive potassium secretion
Protracted vomiting or gastric suction (which removes volume and hydrochloric acid) causes renal potassium losses due to metabolic alkalosis and stimulation of aldosterone due to volume depletion; aldosterone and metabolic alkalosis both cause the kidneys to excrete potassium.
Intracellular shift
The transcellular shift of potassium into cells may also cause hypokalemia. This shift can occur in any of the following:
After administration of insulin
Glycogenesis during parenteral nutrition or enteral hyperalimentation (stimulating insulin release)
Stimulation of the sympathetic nervous system, particularly with beta 2-agonists (eg, albuterol, terbutaline), which may increase cellular potassium uptake
Thyrotoxicosis (occasionally) due to excessive beta-sympathetic stimulation (hypokalemic thyrotoxic periodic paralysis)
Familial periodic paralysis is a rare autosomal dominant disorder characterized by transient episodes of profound hypokalemia thought to be due to sudden abnormal shifts of potassium into cells. Episodes frequently involve varying degrees of paralysis. They are typically precipitated by a large carbohydrate meal or strenuous exercise.
Renal potassium losses
Various disorders can increase renal potassium excretion.
Excess mineralocorticoid (ie, aldosterone) effect can directly increase potassium secretion by the distal nephrons and occurs in any of the following:
Adrenal steroid excess that is due to Cushing syndrome, primary hyperaldosteronism, rare renin-secreting tumors, glucocorticoid-remediable aldosteronism (a rare inherited disorder involving abnormal aldosterone metabolism), or congenital adrenal hyperplasia.
Bartter syndrome, an uncommon genetic disorder that is characterized by renal potassium and sodium wasting, excessive production of renin and aldosterone, and normotension. Bartter syndrome is caused by mutations in a loop diuretic–sensitive ion transport mechanism in the loop of Henle.
Gitelman syndrome is an uncommon genetic disorder characterized by renal potassium and sodium wasting, excessive production of renin and aldosterone, and normotension. Gitelman syndrome is caused by loss of function mutations in a thiazide-sensitive ion transport mechanism in the distal nephron.
Ingestion of substances such as glycyrrhizin (present in natural licorice and used in the manufacture of chewing tobacco), which inhibits the enzyme 11 beta-hydroxysteroid dehydrogenase (11β-HSDH), preventing the conversion of cortisol, which has some mineralocorticoid activity, to cortisone, which does not, resulting in high circulating concentrations of cortisol and renal potassium wasting.
Liddle syndrome, a rare autosomal dominant disorder caused by unrestrained sodium reabsorption in the distal nephron due to one of several mutations found in genes encoding for epithelial sodium channel subunits. Inappropriately high reabsorption of sodium results in both severe hypertension and renal potassium wasting, resulting in hypokalemia.
Renal potassium wasting can also be caused by numerous congenital and acquired renal tubular diseases, such as the renal tubular acidoses and Fanconi syndrome, an unusual syndrome resulting in renal wasting of potassium, glucose, phosphate, uric acid, and amino acids.
Hypomagnesemia is a common correlate of hypokalemia. Much of this correlation is attributable to common causes (ie, diuretics, diarrhea), but hypomagnesemia itself may also result in increased renal potassium losses.
Medications
Diuretics are by far the most commonly used medications that cause hypokalemia. Potassium-wasting diuretics that block sodium reabsorption proximal to the distal nephron include:
Loop diuretics
Osmotic diuretics
Thiazide diuretics
By inducing diarrhea, laxatives, especially when abused, can cause hypokalemia. Surreptitious use of diuretics or laxatives or both is a frequent cause of persistent hypokalemia, particularly among patients preoccupied with weight loss and among health care professionals with access to prescription medications.
Other medications that can cause hypokalemia include:
Amphotericin B
Antipseudomonal penicillin (eg, piperacillin)
Penicillin, in high doses
Theophylline (both acute and chronic intoxication)
Symptoms and Signs of Hypokalemia
Mild hypokalemia (serum potassium 3.0 to 3.4 mEq/L [3.0 to 3.4 mmol/L]) rarely causes symptoms. Moderate hypokalemia (serum potassium 2.5 to 3.0 mEq/L [2.5 to 3.0 mmol/L]) generally causes muscle weakness and may lead to paralysis and respiratory failure. Severe hypokalemia (< 2.5 mEq/L [< 2.5 mmol/L]) causes ECG changes or severe symptoms.
Other muscular dysfunction includes cramping, fasciculations, paralytic ileus, hypoventilation, hypotension, tetany, and rhabdomyolysis.
Persistent hypokalemia can impair renal concentrating ability, causing polyuria with secondary polydipsia.
Diagnosis of Hypokalemia
Serum potassium measurement
ECG
When the mechanism is not evident clinically, measurement of 24-hour urinary potassium excretion and serum magnesium concentration
Hypokalemia (serum potassium < 3.5 mEq/L [< 3.5 mmol/L]) may be found during routine serum electrolyte measurement. It should be suspected in patients with typical changes on an ECG or in those who have muscular symptoms and risk factors. In patients with ECG changes, hypokalemia is confirmed by blood testing.
ECG
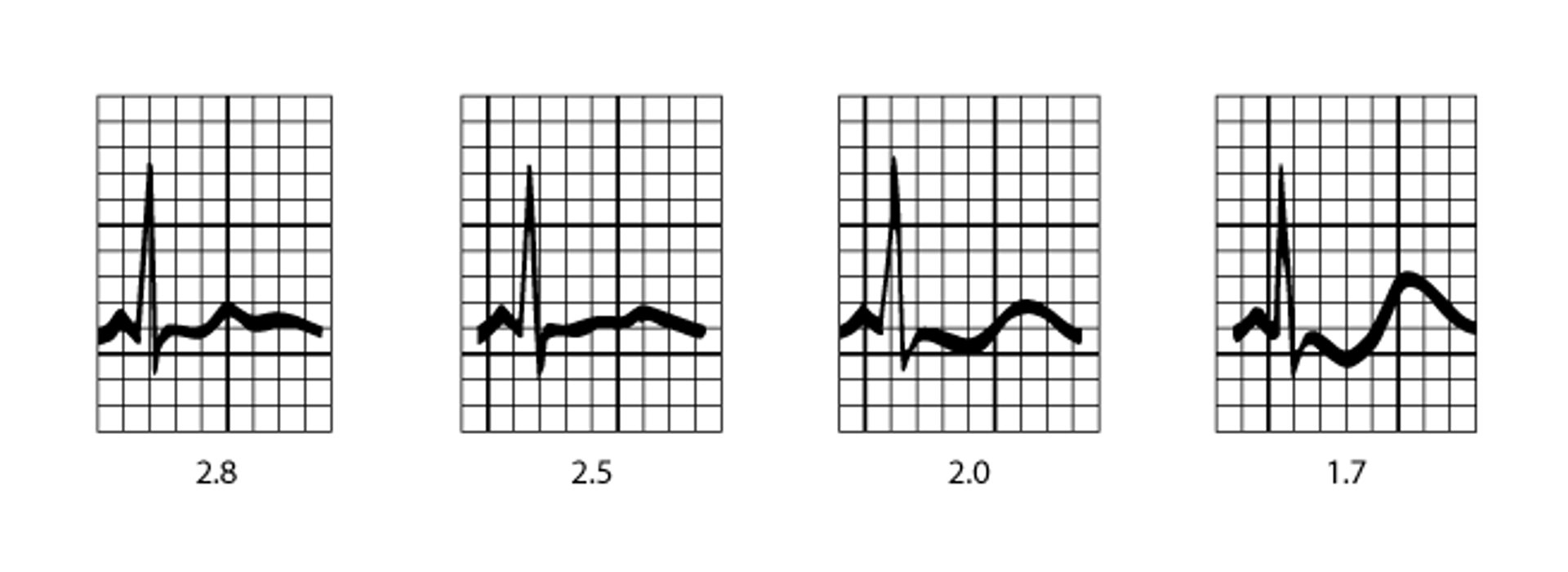
ECG should be done on patients with moderate to severe hypokalemia. Cardiac effects of hypokalemia are usually minimal until serum potassium concentrations are < 3 mEq/L (< 3 mmol/L). Hypokalemia causes sagging of the ST segment, depression of the T wave, and elevation of the U wave. As hypokalemia worsens, the T wave becomes progressively smaller and the U wave becomes increasingly larger. Sometimes, a flat or positive T wave merges with a positive U wave, which may be confused with QT prolongation (see figure ). Hypokalemia may cause premature ventricular beats and premature atrial contractions, ventricular and supraventricular tachyarrhythmias, and second- or third-degree atrioventricular block. Such arrhythmias become more severe with increasingly severe hypokalemia; eventually, ventricular fibrillation may occur. Patients with significant preexisting heart disease and patients receiving digoxin are at risk of cardiac conduction abnormalities as a result of even mild hypokalemia.

ECG Patterns in Hypokalemia
Typical progression of ECG findings in hypokalemia. Serum potassium (in mEq/L and mmol/L) varies widely among patients with similar ECG changes. |

Diagnosis of cause
The cause of hypokalemia is usually apparent by history (particularly the medication history); when it is not, further investigation is warranted.
After acidosis and other causes of intracellular potassium shift (increased beta-adrenergic effect, hyperinsulinemia) have been eliminated, 24-hour urinary potassium and serum magnesium concentrations are measured. In hypokalemia, potassium secretion is normally < 15 mEq/L (< 15 mmol/L).
Extrarenal (GI) potassium loss or decreased potassium ingestion is suspected in chronic unexplained hypokalemia when renal potassium secretion is < 15 mEq/L (< 15 mmol/L). Secretion of > 15 mEq/L (> 15 mmol/L) suggests a renal cause for potassium loss.
Unexplained hypokalemia with increased renal potassium secretion and hypertension suggests an aldosterone-secreting tumor or Liddle syndrome. Unexplained hypokalemia with increased renal potassium loss and normal blood pressure suggests Bartter syndrome or Gitelman syndrome, but hypomagnesemia, surreptitious vomiting, and diuretic abuse are more common and should also be considered.
Treatment of Hypokalemia
Oral potassium supplements
IV potassium supplements for severe hypokalemia or ongoing potassium losses
Many oral potassium supplements are available. Because high single doses can cause GI irritation and occasional bleeding, deficits are usually replaced in divided doses. Liquid potassium chloride given orally elevates concentrations within 1 to 2 hours but has a bitter taste and is tolerated particularly poorly in doses > 25 to 50 mEq (> 25 to 50 mmol). Wax-impregnated potassium chloride preparations are better tolerated. GI bleeding may be even less common with microencapsulated potassium chloride preparations. Several of these preparations contain 8 or 10 mEq/capsule. Because a decrease in serum potassium of 1 mEq/L (1 mmol/L) correlates with approximately a 200- to 400-mEq (200 to 400 mmol) deficit in total body potassium stores, total deficit can be estimated and replaced over a number of days at 20 to 80 mEq (20 to 80 mmol)/day.
When hypokalemia is severe (eg, with ECG changes or severe symptoms), is unresponsive to oral therapy, or occurs in hospitalized patients who are taking digoxin or who have significant heart disease or ongoing losses, potassium must be replaced IV. Because potassium solutions can irritate peripheral veins, the concentration should not exceed 40 mEq/L (40 mmol/L). The rate of correction of hypokalemia is limited because of the lag in potassium movement from the extracellular space into cells. Routine infusion rates should not exceed 10 mEq (10 mmol)/hour.
In hypokalemia-induced arrhythmia, IV potassium chloride must be given more rapidly, usually through a central vein or using multiple peripheral veins simultaneously. Infusion of 40 mEq (40 mmol) potassium chloride/hour can be undertaken but only with continuous cardiac monitoring and hourly serum potassium determinations. Dextrose or glucose solutions used for dilution are avoided because elevation in the serum insulin concentrations could result in transient worsening of hypokalemia.
Even when potassium deficits are severe, it is rarely necessary to give > 100 to 120 mEq (> 100 to 120 mmol) of potassium in a 24-hour period unless potassium loss is ongoing. In potassium deficit with high serum potassium concentration, as in diabetic ketoacidosis, IV potassium is deferred until the serum potassium starts to fall. When hypokalemia occurs with hypomagnesemia, both the potassium and magnesium deficiencies must be corrected to stop ongoing renal potassium wasting.
Prevention of Hypokalemia
Routine potassium replacement is not necessary in most patients receiving diuretics. However, serum potassium should be monitored during diuretic use especially when risk of hypokalemia or its complications is high. Risk is higher in:
Patients with decreased left ventricular function
Patients taking digoxin
Patients with diabetes (in whom insulin concentrations can fluctuate)
Patients with asthma who are taking beta 2-agonists
Potassium sparing diuretics such as triamterene 100 mg orally once a day or spironolactone 25 mg orally 4 times a day do not increase potassium excretion and may be useful in patients who become hypokalemic with other types of diuretics. When hypokalemia develops, potassium supplementation, usually with oral potassium chloride, is indicated.
Key Points
Hypokalemia can be caused by decreased intake of potassium or shift of extracellular potassium into cells, but it is usually caused by excessive losses of potassium in the urine or from the gastrointestinal tract.
Clinical signs include muscle weakness, cramping, fasciculations, paralytic ileus, and when hypokalemia is severe, hypoventilation and hypotension.
ECG changes typically occur when serum potassium is < 3 mEq/L (< 3 mmol/L), and include ST-segment sagging, T wave depression, and U wave elevation. With marked hypokalemia, the T wave becomes progressively smaller and the U wave becomes increasingly larger.
Hypokalemia may cause premature ventricular and atrial contractions, ventricular and atrial tachyarrhythmias, and second- or third-degree atrioventricular block; eventually, ventricular fibrillation may occur.
Replace potassium orally, giving 20 to 80 mEq (20 to 80 mmol)/day unless patients have ECG changes or severe symptoms.
For hypokalemic arrhythmia, give IV potassium chloride through a central vein at a maximum of 40 mEq (40 mmol)/hour and only with continuous cardiac monitoring; routine IV infusion should be no more than 10 mEq (10 mmol)/hour.
Drug Information for the Topic





