



Most genital trauma occurs in males and may involve injury to the testes, scrotum, and/or penis. Genital trauma is the most common genitourinary injury sustained during combat, usually due to ground explosives, and is much less common among civilians. Genital mutilation of females by removing the clitoris, which is done in some cultures, is a form of genital trauma and child abuse.
Most testicular injuries result from blunt trauma (eg, assaults, motor vehicle crashes, sports injuries); penetrating testicular injuries are far less common. Testicular injuries are classified as contusions or, if the tunica albuginea is disrupted, as ruptures.
Isolated scrotal injuries are uncommon and are usually caused by burns, avulsions, or penetrating trauma.
Penile injuries have diverse mechanisms. Zipper injuries are more common in children. Penile fractures, which are ruptures of the corpus cavernosum, occur most often when the penis is forcibly bent during sexual activity and can be accompanied by urethral injury. Amputations (usually self-inflicted or due to clothing trapped by heavy machinery) and strangulations (usually due to constricting penile rings used to enhance erections) are additional mechanisms. Penetrating injuries, including animal and human bites and gunshot wounds, are less common; gunshot wounds often involve the urethra.
Complications of genital injuries include infection, tissue loss, erectile dysfunction, male hypogonadism, and urethral scarring.
Necrotizing genital infections (such as Fournier gangrene) are more likely to occur in people with poorly controlled diabetes or people who are immunocompromised or bedridden.
Symptoms and Signs of Genital Trauma
Symptoms after a direct scrotal blow are usually scrotal pain and swelling. Signs may include scrotal discoloration and a tender, firm scrotal mass that fails to transilluminate, suggesting a hematocele. Scrotal penetration suggests the possibility of testicular involvement. Often the examination is limited by patient discomfort. Penile fractures typically occur during intercourse and result in a cracking sound, immediate pain, marked penile swelling and ecchymosis, and usually a visible deformity. The presence of hematuria suggests the possibility of a concomitant urethral injury.
Necrotizing infections manifest with swelling, crepitus, and fever and progress rapidly to septic shock if not managed promptly and aggressively. A perirectal, periurethral, or cutaneous abscess can often be identified as the initial site of infection.
Diagnosis of Genital Trauma
Clinical evaluation
Ultrasound (for testicular injury)
Retrograde urethrography (for penile injuries with possible urethral involvement)
Diagnosis of external scrotal and penile injuries usually can be made based on physical examination alone. Imaging, such as MRI and ultrasound, can be considered in equivocal cases of penile trauma. A radiograph with urethral contrast (retrograde urethrography) should be done for penile fracture or penetrating penile trauma when urethral injury is suspected (eg, with gross hematuria or inability to void). Clinical diagnosis of testicular contusions and ruptures can be difficult because the degree of injury may be out of proportion to the physical findings, so patients with blunt testicular injury typically require scrotal ultrasound.
Treatment of Genital Trauma
Sometimes surgical repair
Patients with penetrating testicular injuries or clinical or sonographic characteristics that suggest testicular rupture require surgical exploration and repair (1, 2). Similarly, all penile fractures and penetrating injuries should be surgically explored and the defects repaired. Penile amputations should be repaired by microsurgical reimplantation if the amputated segment is viable.
Nonoperative management is appropriate for some genital injuries. Strangulation injuries can usually be managed simply by removing the constricting agent, which may require the use of metal cutters. Animal and human bites involving the genitalia should be managed with copious irrigation, appropriate debridement and antibiotic prophylaxis; primary wound closure is contraindicated. Zipper injuries should be managed by removing the top of the zipper slider (see Zipper removal from penile skin).
Necrotizing scrotal infections require broad-spectrum antibiotic coverage and immediate surgical debridement. Use of a vacuum-assisted closure accelerates healing. Often a cystotomy is required for urinary diversion. Reconstruction is deferred until the infection has resolved and the patient's overall condition has stabilized.
Zipper Removal From Penile Skin

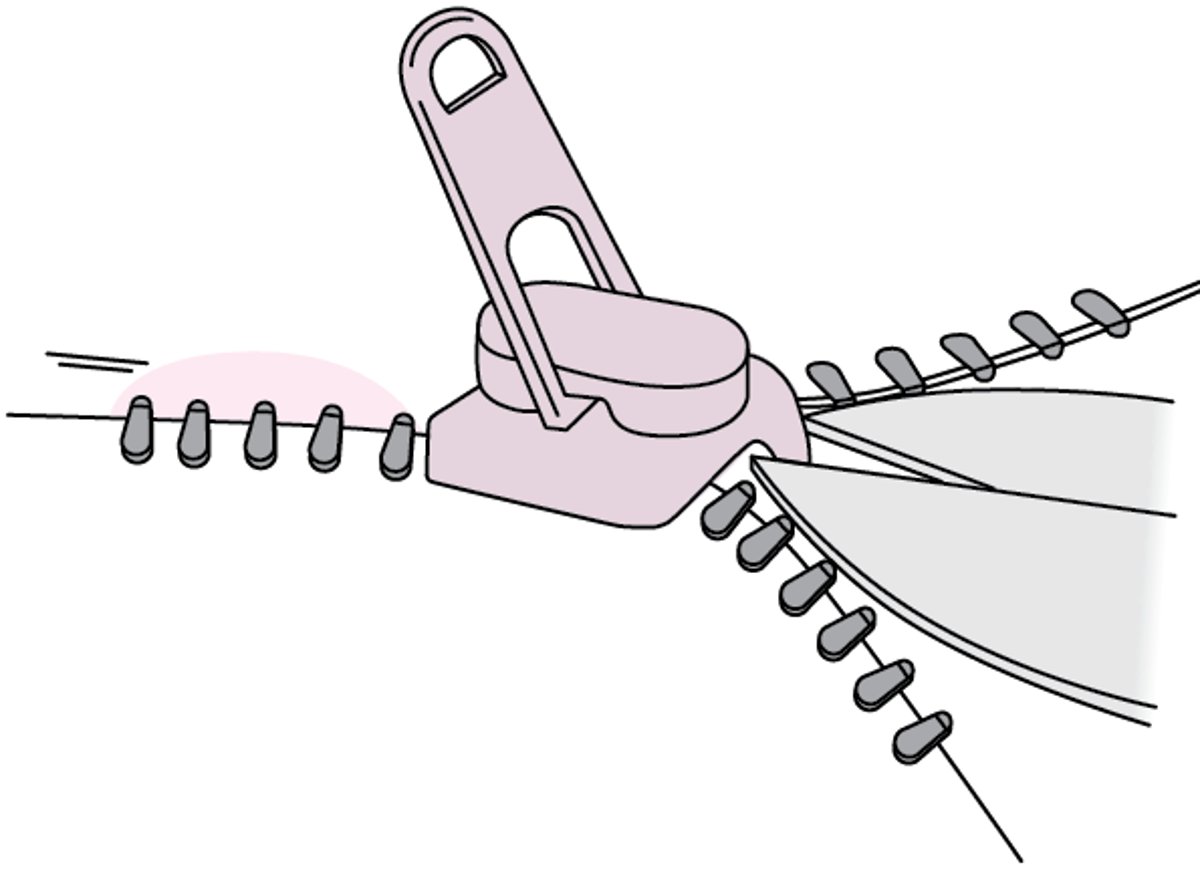
To remove a zipper, inject local anesthetic into the area. Lubricate the zipper with mineral oil and then make one attempt to unzip the zipper. If this attempt is unsuccessful, use a sturdy wire cutter (diagonal cutter) to cut the median bar on the top of the zipper slider, which connects its front and back plates. Then the slider falls off in 2 pieces, and the zipper teeth come apart readily. (For a step-by-step description of the procedure, see How To Remove a Zipper From a Penis.)
Treatment references
1. Morey AF, Broghammer JA, Hollowell CMP, McKibben MJ, Souter L. Urotrauma Guideline 2020: AUA Guideline. J Urol. 2021;205(1):30-35. doi:10.1097/JU.0000000000001408
2. Morey AF, Brandes S, Dugi DD 3rd, et al. Urotrauma: AUA guideline. J Urol. 2014;192(2):327-335. doi:10.1016/j.juro.2014.05.004
Key Points
Diagnose most external scrotal and penile injuries clinically.
Evaluate blunt testicular injuries with ultrasound.
Perform retrograde urethrography to diagnose concomitant urethral injury in patients with either a penile fracture or a penetrating penile injury presenting with hematuria or inability to void.
Surgically repair certain injuries (eg, testicular ruptures, penile fractures, amputations, and penetrating injuries).
Drug Information for the Topic





