

Hypertension is sustained elevation of resting systolic blood pressure (≥ 130 mm Hg), diastolic blood pressure (≥ 80 mm Hg), or both. Hypertension with no known cause (primary hypertension) is most common. Hypertension with an identified cause (secondary hypertension) is usually due to primary aldosteronism. Sleep apnea, chronic kidney disease, or renal artery stenosis are other causes of secondary hypertension. Usually, no symptoms develop unless hypertension is severe or long-standing, which results in target organ damage to the brain, heart, or kidneys. Diagnosis is by sphygmomanometry. Tests may be done to determine cause, assess organ damage, and identify other cardiovascular risk factors. Treatment involves lifestyle changes and medications, including diuretics, angiotensin-converting enzyme (ACE) inhibitors, angiotensin II receptor blockers, and calcium channel blockers.
Hypertension is defined as a systolic blood pressure (BP) ≥ 130 mm Hg or a diastolic blood pressure ≥ 80 mm Hg or taking medication for hypertension. This definition is based on the relationship between blood pressure and cardiovascular events in large populations. Nearly half of adults in the United States have hypertension. Many of these people are not aware that they have hypertension. Approximately 80% of adults with hypertension have been advised to begin treatment with medication and lifestyle modification, but only approximately 50% with hypertension actually receive treatment (1).
Even with medication and lifestyle modification, BP is at goal (under control) in only 26% of patients, and, among treated adults whose BP is not at goal, almost 60% have a BP ≥ 140/90 mm Hg (1).
High blood pressure is more common in non-Hispanic Black adults (58%) than in non-Hispanic White adults (49%), non-Hispanic Asian adults (45%), or Hispanic adults (39%) (1). Among those for whom blood pressure medication and lifestyle modification have been recommended, control of blood pressure is higher among non-Hispanic White adults (31%) than in non-Hispanic Black adults (20%), non-Hispanic Asian adults (24%), or Hispanic adults (23%) (1).
Blood pressure increases with age. About two-thirds of people > 65 years have hypertension, and people with a normal BP at age 55 have a 90% lifetime risk of developing hypertension (2). Although hypertension is common with increased age, treatment remains important because higher BP increases morbidity and mortality risk.
Special considerations are indicated for hypertension during pregnancy because complications are different. Hypertension that develops during pregnancy may resolve after pregnancy (see Hypertension in Pregnancy and Preeclampsia and Eclampsia).
Categories of BP in adults, defined by the American College of Cardiology/American Heart Association (ACC/AHA), include normal, elevated BP, stage 1 (mild) or stage 2 hypertension (3) (see table ). Normal values for blood pressure in infants, children, and adolescents are much lower than those in adults (4).
Classification of Blood Pressure in Adults*
Classification | Blood Pressure |
|---|---|
Normal blood pressure | < 120/80 mm Hg |
Elevated blood pressure | 120–129/< 80 mm Hg |
Stage 1 hypertension | 130–139 mm Hg (systolic) OR 80–89 mm Hg (diastolic) |
Stage 2 hypertension | ≥ 140 mm Hg (systolic) OR ≥ 90 mm Hg (diastolic) |
* Patients with systolic and diastolic blood pressure in different categories should be designated to the higher blood pressure category. | |
Data from Writing Committee Members*, Jones DW, Ferdinand KC, et al. 2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Hypertension. 2025;82(10):e212-e316. doi:10.1161/HYP.0000000000000249 | |
General references
1. Million Hearts. Estimated Hypertension Prevalence, Treatment, and Control Among U.S. Adults. https://millionhearts.hhs.gov/data-reports/hypertension-prevalence.html March 21, 2021. Accessed November 10, 2025. https://millionhearts.hhs.gov/data-reports/hypertension-prevalence.html
2. Vasan RS, Beiser A, Seshadri S, et al. Residual lifetime risk for developing hypertension in middle-aged women and men: The Framingham Heart Study. JAMA. 2002;287(8):1003-1010. doi:10.1001/jama.287.8.1003
3. Writing Committee Members*, Jones DW, Ferdinand KC, et al. 2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Hypertension. 2025;82(10):e212-e316. doi:10.1161/HYP.0000000000000249
4. Flynn J.T, Kaelber DC, Baker-Smith CM, et al; Subcommittee on Screening and Management of High Blood Pressure in Children. Clinical practice guideline for screening and management of high blood pressure in children and adolescents. Pediatrics. 2017;140(3):e20171904. doi:10.1542/peds.2017-3035
Etiology of Hypertension


Hypertension may be:
Primary (no specific cause—85% of cases)
Secondary (an identified cause)
Primary hypertension
Hemodynamics and physiologic components (eg, plasma volume, activity of the renin-angiotensin system) vary, indicating that primary hypertension is unlikely to have a single cause. Even if one factor is recognized, multiple factors are probably involved in sustaining elevated blood pressure (the mosaic theory). Heredity is a predisposing factor, but the exact mechanism by which genetics plays a role is unclear. At younger ages, environmental factors (eg, dietary sodium, stress) seem to affect only people who are genetically susceptible; however, in patients > 65 years, high sodium intake becomes more likely to precipitate hypertension.
Secondary hypertension
Common causes include (1):
Renal parenchymal disease: Chronic glomerulonephritis or pyelonephritis, polycystic renal disease, lupus nephritis, obstructive uropathy
Other endocrine disorders (less common): Pheochromocytoma, Cushing syndrome, congenital adrenal hyperplasia, hyperthyroidism, hypothyroidism (myxedema), primary hyperparathyroidism, acromegaly, and mineralocorticoid excess syndromes other than primary aldosteronism
Prescription or over-the-counter medications: Sympathomimetics (decongestants), nonsteroidal anti-inflammatory drugs (NSAIDs), antipsychotics, tyrosine kinase inhibitors, angiogenesis inhibitors, stimulants, corticosteroids, cocaine
Vascular anomalies: Coarctation of the aorta
Licorice may contribute to worsening of blood pressure control. Diabetes is not considered a cause of secondary hypertension, although patients with diabetes commonly also are hypertensive.
Etiology references
1. Rimoldi SF, Scherrer U, Messerli FH. Secondary arterial hypertension: when, who, and how to screen? Eur Heart J. 2014;35(19):1245–1254. doi:10.1093/eurheartj/eht534
2. Brown JM, Siddiqui M, Calhoun DA, et al. The unrecognized prevalence of primary aldosteronism: A cross-sectional study. Ann Intern Med. 2020;173(1):10–20. doi:10.7326/M20-0065
Pathophysiology of Hypertension
Because blood pressure equals cardiac output (CO) multiplied by total peripheral vascular resistance (TPR), pathogenic mechanisms involve:
Increased CO
Increased TPR
Both
In most patients with hypertension, CO is normal or slightly increased, and TPR is increased. This pattern is typical of primary hypertension and hypertension due to primary aldosteronism, pheochromocytoma, renovascular disease, and renal parenchymal disease.
In other patients, CO is increased (possibly because of venoconstriction in large veins), and TPR is inappropriately normal for the level of CO. Later in the disorder, TPR increases and CO returns to normal, probably because of autoregulation.
Some disorders that increase CO (eg, thyrotoxicosis, arteriovenous fistula, aortic regurgitation), particularly when stroke volume is increased, cause isolated systolic hypertension. Some older patients have isolated systolic hypertension with normal or low CO, probably due to inelasticity of the aorta and its major branches. Patients with high, fixed diastolic pressures often have decreased CO.
Plasma volume tends to decrease as BP increases; rarely, plasma volume remains normal or increases. Plasma volume tends to be high in hypertension due to primary aldosteronism or renal parenchymal disease and may be quite low in hypertension due to pheochromocytoma.
Abnormal sodium transport
In many cases of hypertension, sodium transport across the vascular cell membrane is abnormal, because the sodium-potassium pump (Na+, K+-ATPase) is defective or inhibited, or because permeability to sodium ions is increased. The result is increased intracellular sodium and calcium, which makes the cell more sensitive to sympathetic stimulation. Because Na+, K+-ATPase may pump norepinephrine back into sympathetic neurons (thus inactivating this neurotransmitter), inhibition of this mechanism could also enhance the effect of norepinephrine, increasing BP. Defects in sodium transport may occur in children who are normotensive but have a parent with hypertension.
Sympathetic nervous system
Sympathetic stimulation increases blood pressure, usually more in patients with hypertension than in patients who are normotensive. Whether this hyperresponsiveness resides in the sympathetic nervous system or in the myocardium and vascular smooth muscle is unknown.
A high resting pulse rate, which may result from increased sympathetic nervous activity, is a well-known predictor of hypertension.
In some patients with hypertension, circulating plasma catecholamine levels during rest are higher than normal.
Renin-angiotensin-aldosterone system
The renin-angiotensin-aldosterone system helps regulate blood volume and therefore blood pressure. Renin, an enzyme formed in the juxtaglomerular apparatus, catalyzes conversion of angiotensinogen to angiotensin I. This inactive product is cleaved by angiotensin-converting enzyme (ACE), mainly in the lungs but also in the kidneys and brain, to angiotensin II, a potent vasoconstrictor that also stimulates autonomic centers in the brain to increase sympathetic discharge and stimulates release of aldosterone and vasopressin. Aldosterone causes sodium retention and vasopressin causes water retention, elevating BP. Aldosterone also enhances potassium excretion; low plasma potassium (< 3.5 mEq/L [< 3.5 mmol/L]) increases vasoconstriction through closure of potassium channels.
Renin secretion is controlled by at least 4 mechanisms, which are not mutually exclusive:
A renal vascular receptor responds to changes in tension in the afferent arteriolar wall
A macula densa receptor detects changes in the delivery rate or concentration of sodium chloride in the distal tubule
Circulating angiotensin II has a negative feedback effect on renin secretion
Sympathetic nervous system stimulates renin secretion mediated by beta-receptors (via the renal nerve)
Elevated angiotensin II levels are generally acknowledged to be responsible for renovascular hypertension, at least in the early phase, but the role of the renin-angiotensin-aldosterone system in primary hypertension is not established. However, in patients with African ancestry and older patients with hypertension, renin levels tend to be low (1). Older patients also tend to have low angiotensin II levels, which may be related to a more volume-dependent salt-sensitive form of hypertension.
Hypertension due to chronic renal parenchymal disease (renoprival hypertension) results from the combination of a renin-dependent mechanism and a volume-dependent mechanism. In most cases, increased plasma renin activity is not evident. Hypertension is typically moderate and sensitive to sodium and water balance.
Vasodilator deficiency
Deficiency of a vasodilator (eg, bradykinin, nitric oxide), rather than excess of a vasoconstrictor (eg, angiotensin, norepinephrine), may cause hypertension. Reduction in nitric oxide, due to stiff arteries, occurs with aging, and this reduction contributes to salt sensitivity (ie, lesser amounts of salt ingestion will raise BP) (2). With reduced nitric oxide, a large sodium load (eg, a salty meal) may increase systolic BP by > 10 to 20 mm Hg.
If the kidneys do not produce adequate amounts of vasodilators (because of renal parenchymal disease), blood pressure can increase.
Vasodilators and vasoconstrictors (mainly endothelin) are also produced in endothelial cells. Therefore, endothelial dysfunction greatly affects blood pressure.
Pathology and complications
No pathologic changes occur early in hypertension. Severe or prolonged hypertension damages target organs (primarily the cardiovascular system, brain, and kidneys), increasing risk of:
Coronary artery disease (CAD) and myocardial infarction (MI)
Stroke (particularly hemorrhagic)
Death
Elevated BP levels lead to the development of generalized arteriolosclerosis and acceleration of atherogenesis. Arteriolosclerosis is characterized by medial hypertrophy, hyperplasia, and hyalinization of small arteries (arterioles), notably in the eyes and the kidneys. In the kidneys, the changes narrow the arteriolar lumen, increasing TPR; thus, hypertension leads to more hypertension. Furthermore, once arteries are narrowed, any slight additional shortening of already hypertrophied smooth muscle reduces the lumen to a greater extent than in normal-diameter arteries. These effects may explain why the longer hypertension has existed, the less likely specific treatment (eg, renovascular surgery) for secondary causes is to restore blood pressure to normal. Thus, earlier diagnosis and treatment of even modestly elevated BP (ie, systolic BP of 120 to 129 mm Hg, even if the diastolic BP is in normal range) may provide benefit, especially in younger patients with a family history of hypertension.
Because afterload is increased in patients with elevated BP, the left ventricle gradually hypertrophies, causing diastolic dysfunction. The ventricle eventually dilates, causing dilated cardiomyopathy and heart failure, often worsened by arteriosclerotic coronary artery disease. Thoracic aortic dissection is typically a consequence of hypertension; almost all patients with abdominal aortic aneurysms have hypertension.
Pathophysiology references
1. Williams SF, Nicholas SB, Vaziri ND, Norris KC. African Americans, hypertension and the renin angiotensin system. World J Cardiol. 2014;6(9):878-889. doi:10.4330/wjc.v6.i9.878
2. Fujiwara N, Osanai T, Kamada T, et al. Study on the relationship between plasma nitrite and nitrate level and salt sensitivity in human hypertension: modulation of nitric oxide synthesis by salt intake. Circulation. 2000;101:856–861. doi:10.1161/01.cir.101.8.856
Symptoms and Signs of Hypertension
Hypertension is usually asymptomatic until complications develop in target organs. Even severe hypertension (typically defined as systolic blood pressure ≥ 180 mm Hg and/or diastolic blood pressure ≥ 120 mm Hg) can be asymptomatic (hypertensive urgency). When severe hypertension causes cardiovascular, neurologic, renal, and retinal symptoms (eg, symptomatic coronary atherosclerosis, heart failure, hypertensive encephalopathy, renal failure), it is referred to as a hypertensive emergency.
Retinal changes may include arteriolar narrowing, hemorrhages, exudates and, in patients with encephalopathy, papilledema (hypertensive retinopathy). Changes are classified (according to the Keith-Wagener-Barker classification) into 4 groups with increasingly worse prognosis (1):
Grade 1: Constriction of arterioles only
Grade 2: Constriction and sclerosis of arterioles
Grade 3: Hemorrhages and exudates in addition to vascular changes
Grade 4: Papilledema
Symptoms and signs reference
1. Matsuoka S, Kaneko H, Okada A, et al. Association of retinal atherosclerosis assessed using Keith-Wagener-Barker system with incident heart failure and other atherosclerotic cardiovascular disease: Analysis of 319,501 individuals from the general population. Atherosclerosis. 2022;348:68-74. doi:10.1016/j.atherosclerosis.2022.02.024
Diagnosis of Hypertension
Multiple measurements of BP
Testing to diagnose causes and complications
Hypertension is diagnosed by sphygmomanometry. History, physical examination, and other tests help identify etiology and determine whether target organs are damaged.
Multiple measurements of BP are needed to confirm hypertension because of the inherent variability of blood pressure. Blood pressure typically fluctuates with time of day; in classic diurnal variation, BP is higher by day (especially in the morning) and lower by night. Home blood pressure measurement, using a cuffed device, can help confirm a diagnosis of hypertension (1).
Blood pressure measurement
The blood pressure used for formal diagnosis should be an average of 2 or 3 measurements taken in the office at different times under these conditions:
Patient seated in a chair (not examination table) for > 5 minutes, feet on floor, back supported
Upper limb supported at heart level with no clothing covering the area of cuff placement
No exercise, caffeine, or tobacco use for at least 30 minutes
At the first visit, measure BP in both arms; subsequent measurements should use the arm that gave the higher reading.
A properly sized BP cuff is applied to the upper arm. An appropriately sized cuff covers two-thirds of the biceps; the bladder is long enough to encircle > 80% of the arm, and bladder width equals at least 40% of the arm’s circumference. Thus, patients with obesity usually require large cuffs.
Blood pressure may be measured by either auscultatory or oscillometric devices. Fully automated validated oscillometric devices may be preferred over the auscultatory method as they provide accurate BP measurements and reduce human error (1, 2). For the auscultatory measurement, the clinician inflates the cuff above the expected systolic pressure and gradually releases the air while listening with a stethoscope placed over the brachial artery. As the pressure falls, the pressure at which the first heartbeat is heard is systolic BP. Total disappearance of the sound marks diastolic BP. The same principles are followed to measure BP in a forearm (radial artery) and thigh (popliteal artery). Mechanical devices should be calibrated periodically.
Home blood pressure monitoring, combined with periodic clinician in-office measurements, can improve blood pressure control. However, cuffless home devices (such as smart watches) are not adequately precise, and should not be relied upon (1).
BP is measured in both arms because BP that is > 15 mm Hg higher in one arm than the other requires evaluation of the upper vasculature.
BP is measured in a thigh (with a much larger cuff) to exclude coarctation of the aorta, particularly in patients with diminished or delayed femoral pulses; with coarctation, BP is significantly lower in the legs than in the arms.
Variable measurements and hypertension
White coat hypertension is defined as BP that is elevated in the office but does not meet the criteria for hypertension based on out-of-office readings in untreated patients. The prevalence is approximately 10 to 20% of the population and is more common in children, older adults, and women, as well as those with office-based BP close to the diagnostic threshold.
White coat effect refers to BP that is elevated in the office but is normal during out-of-office readings, among patients who are on treatment for hypertension.
The data about treatment outcomes of patients with white coat hypertension are conflicting. Untreated white coat hypertension seems to be associated with more adverse cardiovascular outcomes compared to normotension. Patients with white coat hypertension have a 3- to 4-fold increased risk of developing sustained hypertension after 7 to 10 years compared to normotensive people (3). White coat effect does not appear to be associated with adverse cardiovascular outcomes.
Masked hypertension is defined as blood pressure that is consistently elevated outside the office, but in which office readings do not meet the criteria for hypertension in untreated people. This group of patients may represent 10 to 30% of the adult population and is more common in men, non-Hispanic Black people, and people with diabetes (4).
Masked hypertension and masked uncontrolled hypertension (in those being treated) are associated with increased cardiovascular risk, with mortality similar to the risk in patients with sustained hypertension (5).
Home or ambulatory BP monitoring is indicated when white coat hypertension or masked hypertension is suspected.
History
The history includes the:
Duration of hypertension and previously recorded BP levels
History or symptoms of coronary artery disease, heart failure, or obstructive sleep apnea
Symptoms of, or personal or family history of, other relevant coexisting disorders (eg, stroke, renal dysfunction, peripheral arterial disease, dyslipidemia, diabetes, gout)
Use of medications that predispose to hypertension (eg, NSAIDs, estrogen-containing oral contraceptives)
Sleep duration
Social history includes exercise levels and use of tobacco, alcohol, and stimulants (including medications and illicit drugs).
A dietary history focuses on intake of salt and stimulants (eg, tea, coffee, caffeine-containing sodas, energy drinks).
Physical examination
The physical examination includes measurement of height, weight, and waist circumference; fundoscopic examination for retinopathy; auscultation for bruits in the neck and abdomen; and a full cardiac, respiratory, and neurologic examination. The abdomen is palpated for kidney enlargement and abdominal masses. Peripheral arterial pulses are evaluated; diminished or delayed femoral pulses suggest aortic coarctation, particularly in patients < 30 years. A unilateral renal artery bruit may be heard in thin patients with renovascular hypertension.
Testing
After hypertension is diagnosed based on blood pressure measurements, testing is needed to:
Detect target-organ damage
Identify cardiovascular risk factors
The more severe the hypertension and the younger the patient, the more extensive is the evaluation. For adults newly diagnosed with hypertension, tests should include (1):
Urinalysis and urinary albumin:creatinine ratio; if abnormal, consider renal ultrasound
Lipid panel, complete metabolic panel (including creatinine or cystatin C, potassium, and calcium), fasting plasma glucose or hemoglobin A1c, thyroid-stimulating hormone
ECG
Sometimes measurement of plasma free metanephrines (to detect pheochromocytoma)
Sometimes a sleep study
Depending on results of the examination and initial tests, other tests may be needed. Basic laboratory testing should be repeated at least annually.
Renal ultrasound to evaluate kidney size may provide useful information if urinalysis detects albuminuria (proteinuria), casts, or microhematuria, or if serum creatinine or cystatin C is elevated.
Patients with hypokalemia unrelated to diuretic use are evaluated for high salt intake and for primary aldosteronism by measuring plasma aldosterone levels and plasma renin activity. Screening for primary aldosteronism is also recommended for patients with resistant hypertension, obstructive sleep apnea, or early stroke (< 40 years) (1). The prevalence of primary aldosteronism is higher than previously recognized, occurring in approximately 10 to 20% of patients with resistant hypertension (6, 7).
On ECG, a broad, notched P-wave indicates atrial hypertrophy and, although nonspecific, may be one of the earliest signs of hypertensive heart disease. Elevated QRS voltage, with or without evidence of ischemia, may occur later and indicates left ventricular hypertrophy (LVH). When LVH is seen on ECG, echocardiography is often done.
If coarctation of the aorta is suspected, echocardiography, chest CT, or MRI can confirm the diagnosis.
Patients with labile, significantly elevated BP and symptoms such as headache, palpitations, tachycardia, excessive perspiration, tremor, and pallor are screened for pheochromocytoma by measuring plasma free metanephrines and for hyperthyroidism, first by measuring thyroid-stimulating hormone (TSH).
A sleep study should be strongly considered in patients whose history suggests sleep apnea.

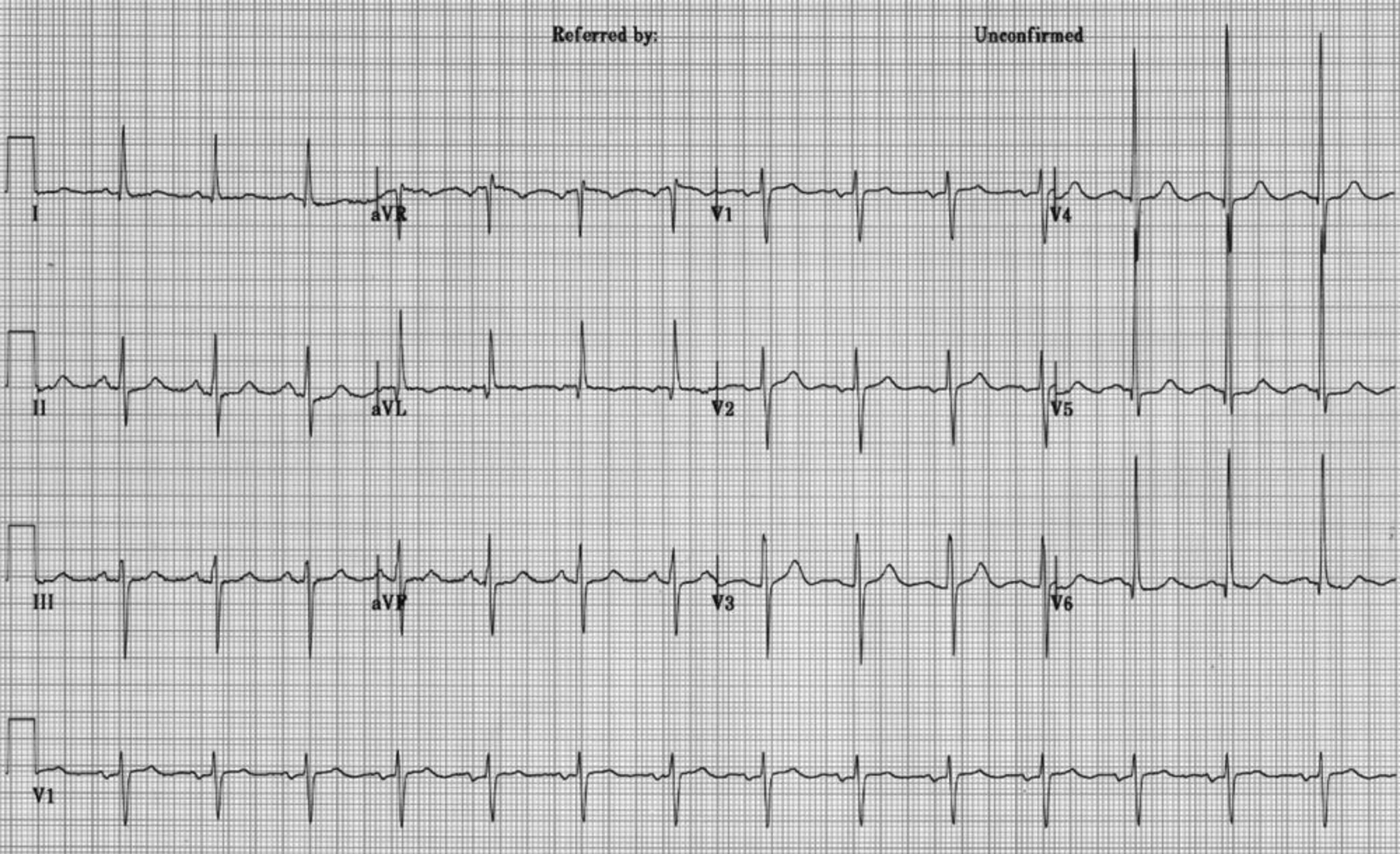
This ECG demonstrates voltage criteria for left ventricular hypertrophy (LVH).
© Springer Science+Business Media
Patients with symptoms suggesting Cushing syndrome, systemic rheumatic diseases, eclampsia, acute porphyria, hyperthyroidism, myxedema, acromegaly, or central nervous system (CNS) disorders also require further evaluation.
Diagnosis references
1. Writing Committee Members*, Jones DW, Ferdinand KC, et al. 2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Hypertension. 2025;82(10):e212-e316. doi:10.1161/HYP.0000000000000249
2. Muntner P, Shimbo D, Carey RM, et al. Measurement of blood pressure in humans: A scientific statement from the American Heart Association. Hypertension. 2019;73:e35–e66. doi:10.1161/HYP.0000000000000087
3. Cohen JB, Lotito MJ, Trivedi UK, Denker MG, Cohen DL, Townsend RR. Cardiovascular events and mortality in white coat hypertension: A systematic review and meta-analysis. Ann Intern Med. 2019;170(12):853–862. doi:10.7326/M19-0223
4. Wang YC, Shimbo D, Muntner P, Moran AE, Krakoff LR, Schwartz JE. Prevalence of masked hypertension among US adults with nonelevated clinic blood pressure. Am J Epidemiol. 2017;185(3):194–202. doi:10.1093/aje/kww237
5. Pierdomenico SD, Pierdomenico AM, Coccina F, et al. Prognostic value of masked uncontrolled hypertension. Hypertension. 2018;72(4):862–869. doi:10.1161/HYPERTENSIONAHA.118.11499
6. Burrello J, Monticone S, Losano I, et al. Prevalence of Hypokalemia and Primary Aldosteronism in 5100 Patients Referred to a Tertiary Hypertension Unit. Hypertension. 2020;75(4):1025-1033. doi:10.1161/HYPERTENSIONAHA.119.14063
7. Mulatero P, Stowasser M, Loh KC, et al. Increased diagnosis of primary aldosteronism, including surgically correctable forms, in centers from five continents. J Clin Endocrinol Metab. 2004;89(3):1045-1050. doi:10.1210/jc.2003-031337
Treatment of Hypertension
Weight loss and exercise
Smoking cessation
Adequate sleep duration (a minimum of 6 hours/night)
Diet: Increased fruits and vegetables, decreased salt, limited alcohol
Medications: Depending on BP and presence of cardiovascular disease or risk factors
Primary hypertension has no cure, but some causes of secondary hypertension can be corrected. In all cases, control of blood pressure can significantly limit adverse consequences.
Goal blood pressure for most patients is
BP < 130/80 mm Hg
Goal pressure in part depends on cardiovascular risk, which is best determined by the PREVENT calculator (1). Patients with a 10-year cardiovascular disease (CVD) risk ≥ 7.5% should be encouraged to achieve a systolic BP < 120 mm Hg (2). BP below 130/80 mm Hg appears to continue to reduce the risk of vascular complications. Even older patients, including frail older patients, can tolerate a diastolic BP as low as 60 to 65 mm Hg without an increase in cardiovascular events (3, 4). However, decreasing systolic pressure increases the risk of adverse medication effects (eg, dizziness, light-headedness, possible worsened renal function), and the benefits of lowering BP to levels < 120 mm Hg systolic should be weighed against risks and patient tolerance.
Ideally, patients or family members measure BP at home, provided they have been trained to do so and the sphygmomanometer is regularly calibrated.
Lifestyle modifications
Lifestyle modifications are recommended for all patients with elevated BP or any stage hypertension (2). The best proven nonpharmacologic interventions for prevention and treatment of hypertension include the following:
Increased physical activity, ideally with a structured exercise program
Weight loss, if appropriate
Healthy diet rich in fruits, vegetables, whole grains, and low-fat dairy products, with reduced saturated and total fat content
Reduced dietary sodium, optimally to < 1500 mg/day (approximately 3.75 g salt) , but at least a 1000 mg/day reduction
Enhanced dietary potassium intake, unless contraindicated due to chronic kidney disease or use of medications that reduce potassium excretion
Moderation in alcohol intake in those who drink alcohol to ≤ 2 drinks daily for men and ≤ 1 drink daily for women (one drink is about 12 oz of beer, 5 oz of wine, or 1.5 oz distilled spirits)
Adequate sleep duration ( a minimum of 6 hours/night) is also recommended. Short sleep duration (typically defined as < 5 or 6 hours per night in adults, has been associated with hypertension (5). For example, studies suggest that optimizing sleep quality and duration (> 6 hours/night) improves blood pressure control in patients with chronic kidney disease (6).
Dietary modifications can also help control diabetes, obesity, and dyslipidemia. Patients with uncomplicated hypertension do not need to restrict their activities as long as blood pressure is controlled.
Medications
(See also Medications for Hypertension.)
The decision to treat with medication is based on the BP level and the presence of atherosclerotic cardiovascular disease (ASCVD) or its risk factors as determined by the PREVENT calculator (1). Patients with a 10-year predicted risk for CVD events ≥ 7.5% using PREVENT are considered to be at increased risk.
Antihypertensive medication should be initiated for patients with hypertension who meet any of the following criteria (2):
Average BP ≥ 140/90 mm Hg
Existing cardiovascular disease (coronary heart disease, stroke, or heart failure) and average BP ≥ 130 mm Hg systolic or ≥ 80 mm Hg diastolic
Diabetes, chronic kidney disease or 10-year PREVENT cardiovascular risk ≥ 7.5% and average BP ≥ 130 mm Hg systolic or ≥ 80 mm Hg diastolic
Persistent average BP ≥ 130 mm Hg systolic or ≥ 80 mm Hg diastolic after 3 to 6 months of lifestyle intervention
An important part of management is continued reassessment. If patients are not at goal BP, clinicians should strive to optimize adherence to the current regimen before switching or adding medications.
Treatment of hypertension during pregnancy requires careful medication selection because some antihypertensive medications can harm the fetus.
Medication selection is based on several factors, including comorbidities, contraindications, and tolerability. For most patients, when selecting an agent for monotherapy, initial treatment may be with any of the following medication classes:
Angiotensin-converting enzyme (ACE) inhibitor
Angiotensin II receptor blocker (ARB)
Dihydropyridine calcium channel blocker
Thiazide diuretic (preferably a thiazide-like diuretic such as chlorthalidone or indapamide)Thiazide diuretic (preferably a thiazide-like diuretic such as chlorthalidone or indapamide)
Adults with stage 1 hypertension (systolic BP 130 to 139/diastolic BP 80 to 89 mm Hg) may be treated initially with a single first-line medication, with dose titration and sequential addition of other medications as needed to achieve blood pressure control (2). Adults with stage 2 hypertension (systolic BP ≥ 140/diastolic BP ≥ 90 mm Hg) should be treated initially with 2 first line medications: an ACE inhibitor or ARB combined with either a diuretic or a calcium channel blocker. When combination therapy is indicated, starting treatment with single pill combinations improves adherence (7, 8).
Signs of hypertensive emergencies require immediate blood pressure reduction with parenteral antihypertensives. Such signs may include seizures or focal neurologic symptoms, retinal hemorrhage, chest pain, dyspnea,or nausea and vomiting.
Some antihypertensives are avoided in certain disorders (eg, ACE inhibitors in severe aortic stenosis) whereas others are preferred for certain disorders (eg, calcium channel blockers for patients with angina pectoris, ACE inhibitors or ARBs for patients with diabetes and proteinuria—see tables and ).
If the goal BP is not achieved within 1 month, assess adherence and tolerability and reinforce the importance of following treatment. If patients are adherent with the regimen, the dose of the initial medication can be increased or a second medication added (selected from among medications recommended for initial treatment). Note that an ACE inhibitor and an ARB should not be used together. Therapy is titrated frequently.
If target BP cannot be achieved with 2 medications, a third medication from choices of initial medications is added. If such a third medication is not tolerated or is contraindicated, a medication from another class (eg, aldosterone antagonist) can be used. Patients with such difficult to control BP may benefit from consultation with a hypertension specialist. For resistant hypertension (BP remains above goal despite use of 3 different antihypertensive medications), 4 or more medications are commonly needed.
Initial Choice of Antihypertensive Medication Class
Medication Class | Indications |
|---|---|
ACE inhibitors* | Youth Left ventricular failure due to systolic dysfunction† Albumin:creatinine ratio > 30 mg/gram (> 33.9 mg/mmol) in patients with chronic renal disorders or diabetic glomerulosclerosis Erectile dysfunction due to other medications |
Angiotensin II receptor blockers* | Youth Conditions for which ACE inhibitors are indicated but not tolerated because of cough or angioedema Diabetes with nephropathy Left ventricular failure with systolic dysfunction Secondary stroke |
Long-acting calcium channel blockers | Older age Arrhythmias (eg, atrial fibrillation, paroxysmal supraventricular tachycardia) Isolated systolic hypertension in older patients (dihydropyridines)† High CAD risk (nondihydropyridines)† |
Thiazide-type diuretics† (chlorthalidone or indapamide)Thiazide-type diuretics† (chlorthalidone or indapamide) | Older age |
* Contraindicated in pregnancy. | |
† Reduced morbidity and mortality rates in randomized studies. | |
ACE = angiotensin-converting enzyme; CAD = coronary artery disease. | |
Achieving adequate blood pressure control often requires several evaluations and changes in pharmacotherapy. Reluctance to titrate or add medications to control BP must be overcome. Nonadherence to therapy, particularly because lifelong treatment is required, can interfere with adequate BP control. Education, with empathy and support, is essential for success.
Antihypertensives for Patients With Comorbidities
Comorbidity | Medication Classes |
|---|---|
ACE inhibitors | |
Diuretics ACE inhibitors Angiotensin II receptor blockers Calcium channel blockers | |
ACE inhibitors Angiotensin II receptor blockers Beta-blockers Other diuretics* | |
ACE inhibitors Beta-blockers Spironolactone or eplerenoneSpironolactone or eplerenone | |
Risk of recurrent stroke | ACE inhibitors Angiotensin II receptor blockers Calcium channel blockers Diuretics |
* Long-term diuretic use may increase mortality in patients with heart failure who do not have pulmonary congestion. | |
ACE = angiotensin-converting enzyme. | |
Devices and physical interventions
Renal artery sympathetic nerve ablation is a potential option for uncontrolled hypertension, using percutaneous catheter-based radiofrequency devices, ultrasound, or the injection of neurolytic agents into tissues surrounding the renal vasculature (9). Several industry-funded sham-controlled studies with different patient populations (eg, untreated hypertension [10], treated hypertension [11], or resistant hypertension [12]) have demonstrated statistically and/or clinically significant reductions in systolic blood pressure. However, whether these devices reduce major cardiovascular events remains uncertain, with studies ongoing related to efficacy, patient selection, safety, and long-term impact on quality of life (13).
Baroreflex activation therapy has been proposed for management of resistant hypertension, but studies have not provided sufficient evidence to recommend the use of these devices (2). The therapy employs a battery-powered device surgically implanted around the carotid body to stimulate the baroreceptor and, in a dose-dependent manner, lower blood pressure. In one long-term follow-up study of patients with resistant hypertension who were included in earlier pivotal trials, baroreflex activation therapy maintained its efficacy for persistent reduction of office BP without major safety issues (14).
Resistant hypertension
Resistant hypertension is defined as blood pressure that is not controlled to goal despite adherence to 3 suitably dosed antihypertensive medications of different classes (including a diuretic) and after white coat effect is excluded. Blood pressure that requires 4 drugs to achieve control is also considered controlled resistant hypertension. Use of a mineralocorticoid receptor antagonist can be beneficial in attaining goal blood pressure (15).
Secondary causes of hypertension must be excluded as part of the evaluation for resistant hypertension. Hyperaldosteronism or subclinical hypercortisolism has been identified in 15 to 20% of cases of resistant hypertension.
Treatment references
1. Khan SS, Coresh J, Pencina MJ, et al. Novel Prediction Equations for Absolute Risk Assessment of Total Cardiovascular Disease Incorporating Cardiovascular-Kidney-Metabolic Health: A Scientific Statement From the American Heart Association. Circulation. 2023;148(24):1982-2004. doi:10.1161/CIR.0000000000001191
2. Writing Committee Members*, Jones DW, Ferdinand KC, et al. 2025 AHA/ACC/AANP/AAPA/ABC/ACCP/ACPM/AGS/AMA/ASPC/NMA/PCNA/SGIM Guideline for the Prevention, Detection, Evaluation and Management of High Blood Pressure in Adults: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Hypertension. 2025;82(10):e212-e316. doi:10.1161/HYP.0000000000000249
3. Williamson JD, Supiano MA, Applegate WB, et al. Intensive vs Standard Blood Pressure Control and Cardiovascular Disease Outcomes in Adults Aged ≥75 Years: A Randomized Clinical Trial. JAMA. 2016;315(24):2673-2682. doi:10.1001/jama.2016.7050
4. White WB, Wakefield DB, Moscufo N, et al. Effects of Intensive Versus Standard Ambulatory Blood Pressure Control on Cerebrovascular Outcomes in Older People (INFINITY). Circulation. 2019;140(20):1626-1635. doi:10.1161/CIRCULATIONAHA.119.041603
Ta
5. Thomas SJ, Calhoun D. Sleep, insomnia, and hypertension: current findings and future directions. J Am Soc Hypertens. 2017;11(2):122-129. doi:10.1016/j.jash.2016.11.008
6. Ali W, Gao G, Bakris GL. Improved Sleep Quality Improves Blood Pressure Control among Patients with Chronic Kidney Disease: A Pilot Study. Am J Nephrol. 2020;51(3):249-254. doi:10.1159/000505895
7. Parati G, Kjeldsen S, Coca A, Cushman WC, Wang J. Adherence to Single-Pill Versus Free-Equivalent Combination Therapy in Hypertension: A Systematic Review and Meta-Analysis. Hypertension. 2012;77(2):692-705. doi:10.1161/HYPERTENSIONAHA.120.15781
8. WilliaMcEvoy JW, McCarthy CP, Bruno RM, et al. 2024 ESC Guidelines for the management of elevated blood pressure and hypertension. Eur Heart J. 2024;45(38):3912-4018. doi:10.1093/eurheartj/ehae178
9. Rey-García J, Townsend RR. Renal Denervation: A Review. Am J Kidney Dis. 2022;80(4):527-535. doi:10.1053/j.ajkd.2022.03.015
10. Böhm M, Kario K, Kandzari DE, et al. Efficacy of catheter-based renal denervation in the absence of antihypertensive medications (SPYRAL HTN-OFF MED Pivotal): a multicentre, randomised, sham-controlled trial. Lancet. 2020;395(10234):1444-1451. doi:10.1016/S0140-6736(20)30554-7
11. Mahfoud F, Kandzari DE, Kario K, et al. Long-term efficacy and safety of renal denervation in the presence of antihypertensive drugs (SPYRAL HTN-ON MED): a randomised, sham-controlled trial. Lancet. 2022;399(10333):1401-1410. doi:10.1016/S0140-6736(22)00455-X
12. Bhatt DL, Vaduganathan M, Kandzari DE, et al. Long-term outcomes after catheter-based renal artery denervation for resistant hypertension: final follow-up of the randomised SYMPLICITY HTN-3 Trial. Lancet. 2022;400(10361):1405-1416. doi:10.1016/S0140-6736(22)01787-1
13. Rao A, Krishnan N. Update on Renal Sympathetic Denervation for the Treatment of Hypertension. Curr Cardiol Rep. 2022;24(10):1261-1271. doi:10.1007/s11886-022-01753-x
14. de Leeuw PW, Bisognano JD, Bakris GL, Nadim MK, Haller H, Kroon AA, DEBuT-T and Rheos Trial Investigators. Sustained reduction of blood pressure with baroreceptor activation therapy: Results of the 6-year open follow-up. Hypertension. 2017;69:836–843. doi:10.1161/HYPERTENSIONAHA.117.09086
15. Carey RM, Calhoun DA, Bakris GL, et al. Resistant hypertension: Detection, evaluation, and management: A Scientific Statement From the American Heart Association. Hypertension. 2018;72:e53–e90. doi: 10.1161/HYP.0000000000000084
Prognosis for Hypertension
The higher the blood pressure, and the more severe the retinal changes and other evidence of target-organ involvement, the worse the prognosis. Systolic BP predicts fatal and nonfatal cardiovascular events better than diastolic BP (1, 2). Effective control of hypertension prevents most complications and prolongs life.
Without treatment, 1-year survival is < 10% in patients with retinal sclerosis, cotton-wool exudates, arteriolar narrowing, and hemorrhage (grade 3 retinopathy) and is < 5% in patients with the same changes plus papilledema (grade 4 retinopathy [3]).
Coronary artery disease is the most common cause of death among treated patients. Ischemic or hemorrhagic stroke is a common consequence of inadequately treated hypertension.
Prognosis references
1. Bourdillon MT, Song RJ, Musa Yola I, Xanthakis V, Vasan RS. Prevalence, Predictors, Progression, and Prognosis of Hypertension Subtypes in the Framingham Heart Study. J Am Heart Assoc. 2022;11(6):e024202. doi:10.1161/JAHA.121.024202
2. Kannel WB, Gordon T, Schwartz MJ. Systolic versus diastolic blood pressure and risk of coronary heart disease. The Framingham study. Am J Cardiol. 1971;27(4):335-346. doi:10.1016/0002-9149(71)90428-0
3. Dziedziak J, Zaleska-Żmijewska A, Szaflik JP, Cudnoch-Jędrzejewska A. Impact of Arterial Hypertension on the Eye: A Review of the Pathogenesis, Diagnostic Methods, and Treatment of Hypertensive Retinopathy. Med Sci Monit. 2022;28:e935135. doi:10.12659/MSM.935135
Key Points
Only about 50% of patients in the United States with hypertension receive treatment, and about one-quarter of those patients have adequate blood pressure (BP) control.
Most hypertension is primary; only 5 to 15% is secondary to another disorder (eg, primary aldosteronism, renal parenchymal disease).
Severe or prolonged hypertension damages the cardiovascular system, brain, and kidneys, increasing risk of myocardial infarction, stroke, and chronic kidney disease.
Hypertension is usually asymptomatic until complications develop in target organs.
When hypertension is newly diagnosed, do a urinalysis, spot urine albumin:creatinine ratio, blood tests (creatinine, potassium, sodium, calcium, fasting plasma glucose, lipid panel, and thyroid-stimulating hormone), and ECG.
Determine the 10-year cardiovascular risk, using the PREVENT calculator.
Reduce BP to < 130/80 mm Hg for most patients..
Patients, including those with a kidney disorder or diabetes, whose 10-year CVD risk is ≥ 7.5% should be encouraged to achieve a systolic BP < 120 mm Hg. A higher target might be appropriate for frail older patients who become symptomatic at lower pressures.
Treatment involves lifestyle changes, especially a low-sodium and higher potassium diet, medication (including thiazide diuretics, angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers, and dihydropyridine calcium channel blockers), and management of secondary causes of hypertension if present.
Drug Information for the Topic





