



In endometriosis, patches of endometrial tissue—normally occurring only in the lining of the uterus (endometrium)—appear outside the uterus.
It is unknown why endometrial tissue becomes misplaced outside the uterus.
Endometriosis can impair fertility and cause pain (particularly before and during menstrual periods and during sexual intercourse), but it may cause no symptoms.
Usually, doctors check for endometrial tissue by inserting a thin viewing tube through a small incision near the navel (laparoscopy).
Medications are used to relieve pain and to slow the growth of the misplaced tissue.
Surgery may be done to remove the misplaced endometrial tissue and sometimes to remove the uterus and the ovaries.
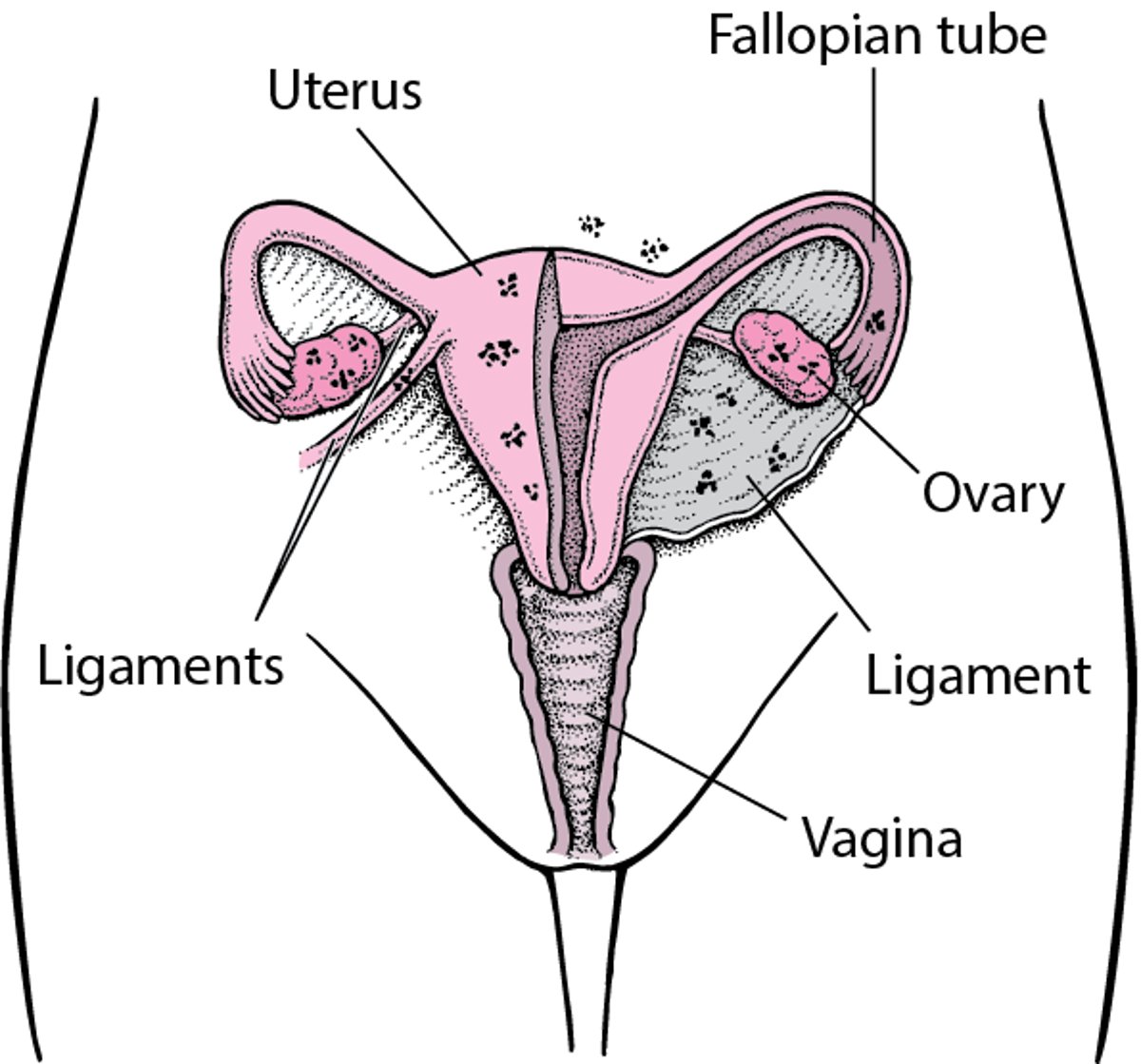
Endometriosis: Misplaced Tissue
In endometriosis, small or large patches of endometrial tissue, which is usually located only in the lining of the uterus (endometrium), appear in other parts of the body. How and why the tissue appears in other locations is unclear. Common locations of misplaced endometrial tissue include the ovaries and ligaments supporting the uterus and, less commonly, the fallopian tubes. But the misplaced tissue may also appear in other locations in the pelvis and abdomen or, rarely, on the membranes that cover the lungs or heart. The misplaced endometrial tissue can irritate nearby tissues, causing bands of scar tissue (adhesions) to form between structures in the abdomen. The misplaced tissue can also block the fallopian tubes, causing infertility. |

Endometriosis is a chronic disorder that may be painful. It is unknown exactly how many women have endometriosis because it can usually be diagnosed only by directly viewing the tissue inside the uterus (endometrial tissue), which requires a surgical procedure, typically laparoscopy. About 18% of all women are diagnosed with endometriosis. The percentage of women who have endometriosis is higher among women who have infertility (about 30%) and women who have chronic pelvic pain (about 40%). The average age at diagnosis is 28, but endometriosis can develop in adolescents and, rarely, young girls.
Common locations of misplaced endometrial tissue (called implants) include the following:
Ovaries
Ligaments that support the uterus
Tissue that lines the inside of the abdomen and pelvis (peritoneum)
Less common locations include the fallopian tubes, the outer surface of the small and large intestines, the ureters (tubes leading from the kidneys to the bladder), the bladder, the space between the vagina and rectum, and the vagina. Rarely, endometrial tissue grows on the membranes covering the lungs (pleura), the sac that envelops the heart (pericardium), the vulva, the cervix, or surgical scars in the abdomen.
The misplaced endometrial tissue responds to hormones as normal endometrial tissue does during the menstrual cycle. Thus, endometrial implants can bleed and cause pain, particularly before and during menstrual periods. The severity of symptoms and the disorder's effects on fertility and on organ function vary greatly from woman to woman.
As the disorder progresses, the misplaced endometrial tissue tends to gradually increase in size. It may also spread to new locations. However, how much tissue is present and how quickly endometriosis progresses vary greatly. The tissue may remain on the surface of structures or may penetrate deeply (invade) and form nodules.


Causes of Endometriosis
The cause of endometriosis is unclear, but there are several theories:
Small pieces of the lining of the uterus (endometrium) that are shed during menstruation may flow backward through the fallopian tubes toward the ovaries into the abdominal cavity, rather than flow through the vagina and out of the body with the menstrual period.
Cells from the endometrium (endometrial cells) may be transported through the blood or lymphatic vessels to another location.
Cells located outside the uterus may change into endometrial cells.
Endometriosis sometimes runs in families and is more common among first-degree relatives —mothers, sisters , and children—of women with endometriosis. It is more likely to occur in women with the following characteristics:
Have their first baby after age 30
Have never had a baby
Started to menstruate earlier than usual or stopped menstruating later than usual
Have short menstrual cycles (less than 27 days long) with heavy periods that last more than 8 days
Have certain structural abnormalities of the uterus
Have mothers who, when pregnant, took the medication diethylstilbestrol (DES), prescribed to prevent miscarriage (in 1971, the medication was banned in the United States)
Endometriosis seems to occur less often in women with the following characteristics:
Have had several pregnancies
Started to menstruate later than usual
Breastfeed a long time
Have used low-dose oral contraceptives for a long time
Exercise regularly (especially if they started before age 15, exercise more than 4 hours a week, or both)
Symptoms of Endometriosis
The 3 classic symptoms of endometriosis are pain during the menstrual cycle, pain during sexual intercourse (the pain is usually deep in the belly, not in the surface tissue of the vagina), and infertility. Women may also have pain in the lower abdomen and pelvic area (pelvic pain) not related to the menstrual cycle.
The severity of endometriosis symptoms does not depend on the amount of misplaced endometrial tissue. Some women with a large amount of tissue have no symptoms. Others, even some with a small amount, have incapacitating pain. In many women, endometriosis does not cause pain until it has been present for several years. For some women, sexual intercourse tends to be painful, especially before or during menstruation.
The pain usually varies during the menstrual cycle, worsening before and during menstrual periods. Menstrual irregularities, such as heavy menstrual bleeding and spotting before menstrual periods, may occur. Misplaced endometrial tissue responds to the same hormones—estrogen and progesterone (produced by the ovaries)—as normal endometrial tissue in the uterus. Consequently, the misplaced tissue may bleed during menstruation and cause inflammation. The misplaced tissue often causes cramps and pain.
Symptoms also vary depending on where the endometrial tissue is located. Possible symptoms by location include
Ovaries: Formation of a blood-filled mass (endometrioma), which, if it bursts open, leaks, or twists, may cause pain and sometimes nausea and vomiting
Large intestine: Abdominal bloating, pain during bowel movements, diarrhea or constipation, or rectal bleeding during menstruation
Bladder: Pain above the pubic bone, pain during urination, urine that contains blood, and a frequent and urgent need to urinate
The misplaced endometrial tissue and its bleeding may irritate nearby tissues. As a result, scar tissue may form, sometimes as bands of fibrous tissue (adhesions) between structures in the abdomen. The misplaced endometrial tissue and adhesions can interfere with the functioning of organs. Rarely, adhesions block the intestine.
Severe endometriosis may cause infertility when the misplaced tissue or the scar tissues caused by it block the egg's passage from the ovary into the uterus. Mild endometriosis may also cause infertility, but it is not clear how it does so.
During pregnancy, endometriosis may become inactive (go into remission) temporarily or sometimes permanently. Endometriosis tends to become inactive after menopause because estrogen and progesterone levels decrease.
Diagnosis of Endometriosis
Laparoscopy, sometimes with biopsy, to check for endometrial tissue
Sometimes pelvic ultrasound or magnetic resonance imaging (MRI)
A doctor may suspect endometriosis in a woman who has typical symptoms or unexplained infertility. Occasionally, during a pelvic examination, a woman may feel pain or tenderness, or a doctor may feel a lump or mass of tissue behind the uterus or near the ovaries.
Imaging tests may not reliably detect endometriosis. However, a pelvic ultrasound or MRI may show an ovarian cyst that could be caused by endometriosis (endometrioma) and may help doctors evaluate endometriosis in a noninvasive way (that is, no incision is required). MRI can sometimes detect unique signals that are characteristic of endometrial tissue but cannot detect small patches of endometrial tissue.
To diagnose endometriosis, a doctor examines the abdominal cavity with a thin viewing tube (called a laparoscope) to see whether endometrial tissue is present. The laparoscope is inserted into the abdominal cavity (the space around the abdominal organs) through a small incision most often made just above or below the navel. The abdominal cavity is then inflated with carbon dioxide gas, which distends it and makes the organs easier to see. The entire abdominal cavity is examined.
Laparoscopy is done in a hospital and usually requires a general anesthetic. An overnight stay in the hospital is usually not required. Laparoscopy causes mild to moderate abdominal discomfort, but normal activities can usually be resumed in a few days.
A biopsy is not required to make the diagnosis if a doctor sees abnormal tissue during laparoscopy, but biopsy results confirm the diagnosis. For the biopsy, a sample of the tissue is removed, using instruments inserted through the laparoscope. The sample is then examined using a microscope. An overnight stay in the hospital is usually required only if a very large amount of abnormal tissue is removed.
Depending on the location of the misplaced tissue, a biopsy may be done when the vagina is inspected during a pelvic examination or when a flexible viewing tube is inserted through the anus to examine the lower part of the large intestine, rectum, and anus (sigmoidoscopy) or bladder (cystoscopy). Occasionally, a larger incision in the abdomen (called laparotomy) is required.
Doctors classify endometriosis as minimal (stage I), mild (stage II), moderate (stage III), or severe (stage IV) based on the following:
The amount of misplaced tissue
Its location
Its depth (whether it is on the surface of or deep within an organ)
The presence and number of endometriomas and adhesions
If a woman has infertility, tests may be done to determine whether the cause is endometriosis or another disorder, such as problems with the fallopian tubes.
Treatment of Endometriosis
Nonsteroidal anti-inflammatory drugs for pain
Medications to suppress the activity of the ovaries
Surgery to remove or destroy the misplaced endometrial tissue
Sometimes surgery to remove only the uterus or the uterus and the ovaries
Endometriosis treatment depends on a woman's symptoms, pregnancy plans, and age, as well as the stage of endometriosis.
Medications used to treat endometriosis
Usually, nonsteroidal anti-inflammatory drugs (NSAIDs) are used to relieve pain. They may be all that is needed if symptoms are mild and women do not plan to become pregnant.
Hormonal contraceptives can be used to suppress the activity of the ovaries and thus slow the growth of the misplaced endometrial tissue and reduce bleeding and pain. Hormonal contraceptives are used primarily in women who do not plan to become pregnant soon. The oral contraceptives can be taken continuously, especially if pain is worse during menstrual periods. The following medications are commonly used:
Combination oral contraceptives (estrogen plus a progestin)
Progestins, for women who have cannot have estrogen therapy
The following medications are usually used only if symptoms are not well controlled with NSAIDs or hormonal contraceptives:
Gonadotropin-releasing hormone agonists (GnRH agonists—such as leuprolide)Gonadotropin-releasing hormone agonists (GnRH agonists—such as leuprolide)
GnRH antagonists (such as elagolix or relugolix)GnRH antagonists (such as elagolix or relugolix)
Aromatase inhibitors (such as anastrozole or letrozole)Aromatase inhibitors (such as anastrozole or letrozole)
Danazol (a synthetic male hormone, or androgen)Danazol (a synthetic male hormone, or androgen)
However, these medications may not eliminate endometriosis, and even if they do, endometriosis often recurs after the medications are stopped unless more radical treatment is used to completely and permanently stop the ovaries from functioning.
GnRH agonists turn off the brain's signal to the ovaries to produce estrogen and progesterone. As a result, production of these hormones decreases. Side effects of GnRH agonists include hot flashes, stiff joints, mood changes, and vaginal dryness. Continued use of GnRH agonists for more than 4 to 6 months causes a decrease in bone density and may lead to osteoporosis. To minimize the decrease in bone density, doctors may give women small doses of a progestin or a bisphosphonate (such as alendronate, ibandronate, or risedronate). If endometriosis recurs, women may need to be treated again.. To minimize the decrease in bone density, doctors may give women small doses of a progestin or a bisphosphonate (such as alendronate, ibandronate, or risedronate). If endometriosis recurs, women may need to be treated again.
The GnRH antagonist elagolix, like GnRH agonists, suppresses elagolix, like GnRH agonists, suppressesestrogen production by the ovaries and, if it is taken for a long time, causes a decrease in bone density. If it is taken for more than 6 months, doctors may give women small doses of a progestin to minimize the decrease in bone density.
Relugolix (another GnRH antagonist) combined with estradiol and norethindrone is being studied as a treatment for endometriosis. This combination minimizes hot flushes and bone loss, but if it is taken for more than 24 months, bone loss may continue and may be irreversible.Relugolix (another GnRH antagonist) combined with estradiol and norethindrone is being studied as a treatment for endometriosis. This combination minimizes hot flushes and bone loss, but if it is taken for more than 24 months, bone loss may continue and may be irreversible.
Aromatase inhibitors can be used when GnRH analogs are ineffective in suppressing endometriosis.
DanazolDanazol inhibits release of an egg (ovulation). However, it has side effects including weight gain and the development of masculine characteristics (such as increased body hair, loss of hair from the head, reduced breast size, and lowering of the voice). These side effects limit its use.
Oral contraceptives may be used after treatment with danazol or a GnRH agonist to try to slow progression of endometriosis and to reduce pain. Oral contraceptives may be used after treatment with danazol or a GnRH agonist to try to slow progression of endometriosis and to reduce pain.
Endometriosis surgery
For most women with moderate to severe endometriosis, the most effective treatment is removing or destroying misplaced endometrial tissue and endometriomas. Usually, these surgical procedures are done through a laparoscope inserted into the abdomen through a small incision made near the navel. Such treatment may be needed when
Medications cannot relieve severe lower abdominal or pelvic pain
Adhesions in the lower abdomen or pelvis cause significant symptoms
Misplaced endometrial tissue blocks one or both fallopian tubes
Endometriomas are present
Endometriosis causes infertility and the woman wants to be able to become pregnant
Endometriosis causes pain during intercourse
Often, misplaced endometrial tissue can be removed or destroyed during laparoscopy when the diagnosis is made. Sometimes electrocautery (a device that uses an electrical current to produce heat) or a laser is used to destroy or remove endometrial tissue during laparoscopy. Sometimes abdominal surgery (involving an incision into the abdomen) is required to remove endometrial tissue.
Endometriomas (ovarian cysts caused by endometriosis) are usually removed because they are less likely to recur if they are removed than if they are drained.
During surgery, doctors remove as much misplaced endometrial tissue as possible without damaging the ovaries. Thus, the woman's ability to have children may be preserved. After surgery, fertility rates increase. If doctors cannot remove all of the tissue, women may be treated with a GnRH agonist. But whether this medication increases their chances of becoming pregnant is unclear. Some women who have endometriosis can become pregnant by using assisted reproductive techniques, such as in vitro fertilization.
Surgical removal of misplaced endometrial tissue is only a temporary measure. After the tissue is removed, endometriosis recurs in most women unless they take medications to suppress the ovaries or the ovaries are removed.
Removal of the uterus but not the ovaries (hysterectomy without salpingo-oophorectomy) is often appropriate in women who do not plan to become pregnant, particularly when medications do not relieve abdominal or pelvic pain.
Sometimes both ovaries must be removed, as well as the uterus. This procedure is called hysterectomy plus bilateral salpingo-oophorectomy. It has the same effects as menopause because it, like menopause, results in decreased estrogen levels. Thus, women under 50 years old may be given estrogen to reduce the severity of the menopausal symptoms that occur after this surgery. Most of these women are also given a progestin. The progestin is included to help prevent any remaining misplaced endometrial tissue from growing. A progestin alone can be given to women over 50 to reduce symptoms that persist after the ovaries are removed.
Hysterectomy plus bilateral salpingo-oophorectomy may be done, for example, in the following situations:
When women, usually those who are near menopause or who do not want to become pregnant again, want definitive treatment (to completely eliminate the disorder)
When endometriosis has recurred, often many times
Drug Information for the Topic





