

Auscultation of the heart requires excellent hearing ,experience, and the ability to distinguish subtle differences in pitch and timing. Hearing-impaired health care professionals can use amplified stethoscopes. High-pitched sounds are best heard with the diaphragm of the stethoscope. Low-pitched sounds are best heard with the bell. Very little pressure should be exerted when using the bell. Excessive pressure converts the underlying skin into a diaphragm and eliminates very low-pitched sounds.
The entire precordium is examined systematically, typically beginning over the apical impulse with the patient in the left lateral decubitus position (1). The patient rolls supine, and auscultation continues at the lower left sternal border, proceeds cephalad with auscultation of each interspace, then caudad from the right upper sternal border. The clinician also listens over the left axilla and above the clavicles. The patient sits upright for auscultation of the back, then leans forward to aid auscultation of aortic and pulmonic diastolic murmurs or pericardial friction rub.
Major auscultatory findings include:
Heart sounds
Gallops
Murmurs
Rubs
Heart sounds are brief, transient sounds produced by valve opening and closure; they are divided into systolic and diastolic sounds.
Gallops are diastolic sounds (third heart sound [S3] and fourth heart sound [S4]) caused by ventricular filling; a gallop is usually, but not always, abnormal.
Murmurs are produced by blood flow turbulence and are more prolonged than heart sounds; they may be systolic, diastolic, or continuous. They are graded by intensity and are described by their location and when they occur within the cardiac cycle. Systolic murmurs are graded in intensity on a scale of 1 to 6 (see table ), while diastolic murmurs are graded on a scale of 1 to 4.
Systolic Heart Murmur Intensity
Grade | Description |
|---|---|
1 | Barely audible |
2 | Soft but easily heard |
3 | Loud, without a thrill (a palpable buzzing sensation) |
4 | Loud, with a thrill |
5 | Loud, audible with minimal contact between stethoscope and chest |
6 | Loud, audible with no contact between stethoscope and chest |
Rubs are high-pitched, scratchy sounds often with 2 or 3 separate components, which may vary according to body position; during tachycardia, the sound may be almost continuous.
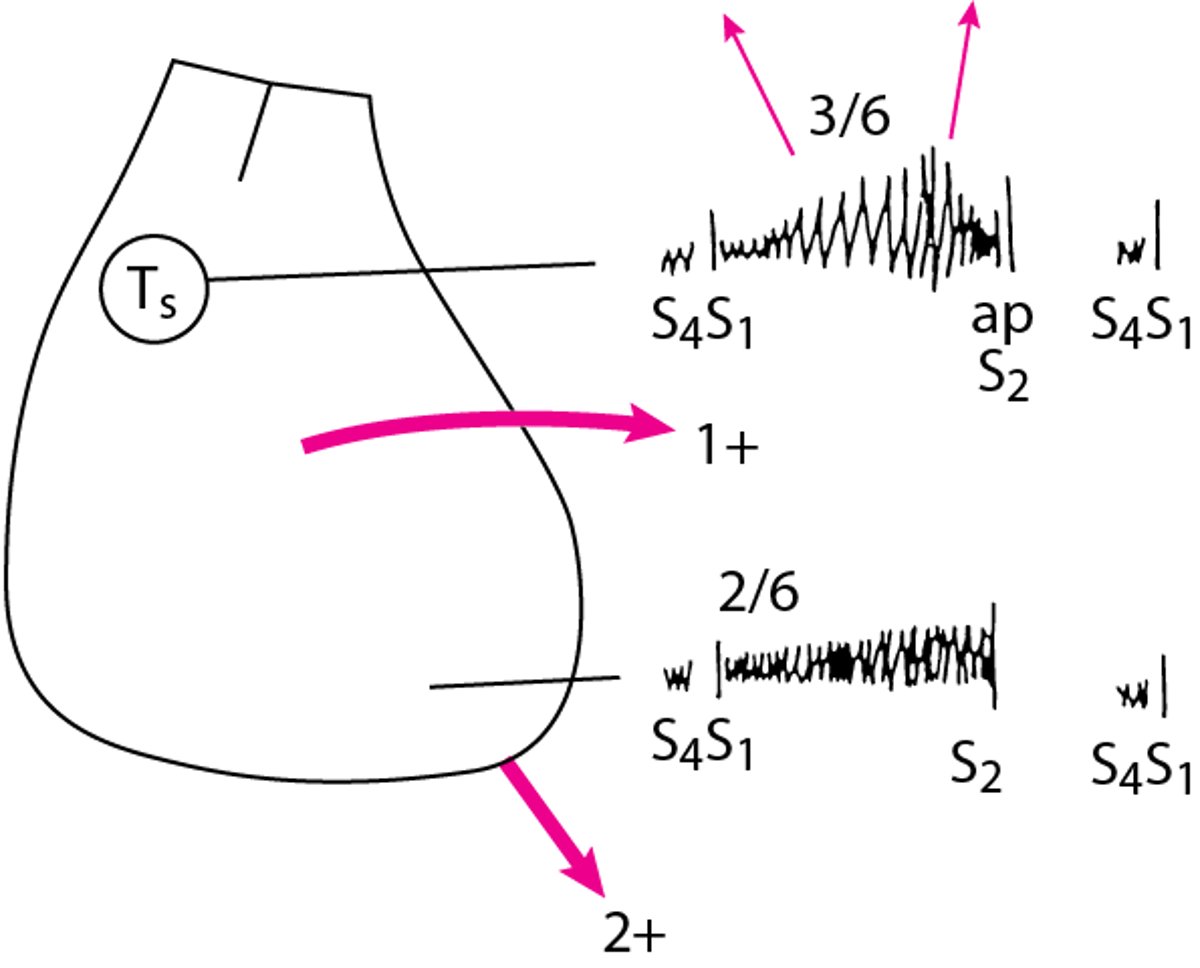
The clinician focuses attention sequentially on each phase of the cardiac cycle, noting each heart sound and murmur. Intensity, pitch, duration, and timing of the sounds and the intervals between them are analyzed, often providing an accurate diagnosis. Historically, a diagram of the major auscultatory and palpatory findings of the precordium was drawn in the patient’s chart each time the patient’s cardiovascular system was examined (see figure ). With such diagrams, findings from each examination could be compared. Subsequent examination findings should be interpreted in the context of available imaging results (including echocardiogram and cardiac MRI) to diagnose and monitor valvular and other abnormalities.
Diagram of Physical Findings in a Patient With Aortic Stenosis and Mitral Regurgitation
Murmur, character, intensity, and radiation are depicted. Sound of pulmonic closure exceeds that of aortic closure. Left ventricular (LV) thrust and right ventricular (RV) lift (heavy arrows) are identified. A fourth heart sound (S4) and systolic thrill (TS) are present. a = aortic closure sound; p = pulmonic closure sound; S1 = first heart sound; S2 = second heart sound; 3/6 = grade of crescendo-diminuendo murmur (radiates to both sides of neck); 2/6 =grade of pansystolic apical crescendo murmur; 1+ = mild precordial lift of RV hypertrophy (arrow shows direction of lift); 2 += moderate LV thrust (arrow shows direction of thrust). |

Systolic heart sounds
Systolic sounds include the following:
First heart sound (S1)
Clicks
S1 and the second heart sound (S2, a diastolic heart sound) are normal components of the cardiac cycle, the familiar “lub-dub” sounds.
S1 occurs just after the beginning of systole and is predominantly due to mitral closure but may also include tricuspid closure components. It is often split and has a high pitch. S1 is loud in mitral stenosis. It may be soft or absent in mitral regurgitation due to valve leaflet sclerosis and rigidity but is often distinctly heard in mitral regurgitation due to myxomatous degeneration of the mitral apparatus or due to ventricular myocardial abnormality (eg, papillary muscle dysfunction, ventricular dilation). S1 is often soft or absent in first-degree atrioventricular block as the atrioventricular valve leaflets (mitral and tricuspid) drift to a nearly closed position prior to ventricular systole.
Clicks occur only during systole; they are distinguished from S1 and S2 by their higher pitch and briefer duration. Some clicks occur at different times during systole as hemodynamics change. Clicks may be single or multiple.
Clicks in congenital aortic stenosis or pulmonic stenosis are thought to result from abnormal ventricular wall tension. These clicks occur early in systole (very near S1) and are not affected by hemodynamic changes. Similar clicks occur in severe pulmonary hypertension. Clicks in mitral valve prolapse or tricuspid valve prolapse, typically occurring in mid to late systole, are thought to result from abnormal tension on redundant and elongated chordae tendineae or valve leaflets.
Clicks due to myxomatous degeneration of valves may occur any time during systole but move toward S1 during maneuvers that transiently decrease ventricular filling volume (eg, standing, Valsalva maneuver). If ventricular filling volume is increased (eg, by lying supine), clicks move toward S2, particularly in mitral valve prolapse. For unknown reasons, characteristics of the clicks may vary greatly between examinations, and clicks may come and go.

S1 splitting is normal in many patients and is thought to be caused by mitral valve closure followed by an aortic eject
Recording provided by Jules Constant, MD.
High pulmonary artery pressures may dilate the pulmonary artery, stretching the valve ring and causing a click when tau
Recording provided by Jules Constant, MD.
Sound is that of S1–S2 with expiration (“out”) and S1–A2–P2 with inspiration (“in”). S2 splits with inspiration because
Recording provided by Jules Constant, MD.
S1 splitting is normal in many patients and is thought to be caused by mitral valve closure followed by an aortic ejection sound.
Recording provided by Jules Constant, MD.
High pulmonary artery pressures may dilate the pulmonary artery, stretching the valve ring and causing a click when taut cusps open rapidly.
Recording provided by Jules Constant, MD.
Sound is that of S1–S2 with expiration (“out”) and S1–A2–P2 with inspiration (“in”). S2 splits with inspiration because intrathoracic pressure decreases, drawing more blood into the right ventricle and postponing pulmonic valve closure.
Recording provided by Jules Constant, MD.
Diastolic heart sounds
Diastolic sounds include the following:
Second, third, and fourth heart sounds (S2, S3, and S4)
Diastolic knocks
Mitral valve sounds
Unlike systolic sounds, diastolic sounds are low-pitched; they are softer in intensity and longer in duration. Except for S2, these sounds are usually abnormal in adults, although an S3 may be physiologic up to age 40 years and during pregnancy.
S2 occurs at the beginning of diastole, and includes aortic and pulmonic valve closure. Normally, aortic valve closure (A2) precedes pulmonic valve closure (P2), with a greater delay in P2 during inspiration due to increased right ventricular filling. When P2 is delayed enough to be audibly distinct from A2, it produces splitting of S2. The change in this delay with respiration causes physiologic splitting of S2, with the split typically audible only during inspiration.
In some conditions in which pulmonic valve closure is delayed (eg, complete right bundle branch block, pulmonic valve stenosis), S2 is widely split but still varies with the respiratory cycle. With an atrial septal defect of the common secundum type, P2 is delayed but does not vary with respiration, resulting in a wide fixed split of S2. Left-to-right shunts with normal right ventricular volume (eg, ventricular septal defects) do not cause fixed splitting.
If aortic valve closure is late (as in left bundle branch block or aortic stenosis), S2 may split in expiration and be single in inspiration when the delayed P2 occurs at the same time as the delayed A2; this is known as paradoxical splitting. Finally, a single S2 may occur when the aortic valve is regurgitant, severely stenotic, or atretic (or in truncus arteriosus when there is a single common valve).
Sound is that of paradoxical splitting, ie, S1–P2–A2 at rest (“out”) and S1–S2 with inspiration (“in”). Left bundle bra
Recording provided by Jules Constant, MD.
Sound is that of wide splitting, ie, S1–A2–P2 at rest (“out”) with an even wider A2–P2 interval with inspiration (“in”)
Recording provided by Jules Constant, MD.
Sound is that of fixed second heart sound (S2) splitting, ie, S1–A2–P2 at rest (“out”) and with inspiration (“in”). Spl
Recording provided by Jules Constant, MD.
Sound is that of S1–S2–S3.
Recording provided by Jules Constant, MD.
Sound is that of S4–S1–S2.
Recording provided by Jules Constant, MD.
Sound is that of S4–S1–S2–S3 in rapid succession.
Recording provided by Jules Constant, MD.
A diastolic knock is a loud third heart sound (S3) caused by constrictive pericarditis.
Recording provided by Jules Constant, MD.
Sound is that of S1–A2–OS with a relatively long A2–OS interval. The opening snap (OS), most commonly caused by mitral
Recording provided by Jules Constant, MD.
Sound is that of paradoxical splitting, ie, S1–P2–A2 at rest (“out”) and S1–S2 with inspiration (“in”). Left bundle branch block delays aortic valve closure, so that split is audible at rest; inspiration decreases intrathoracic pressure, drawing more blood into the right ventricle and postponing pulmonic valve closure until it is superimposed on A2 and splitting becomes inaudible.
Recording provided by Jules Constant, MD.
Sound is that of wide splitting, ie, S1–A2–P2 at rest (“out”) with an even wider A2–P2 interval with inspiration (“in”). Right bundle branch block delays pulmonic valve closure so that S2 splitting becomes audible at rest. Inspiration decreases intrathoracic pressure, drawing more blood into the right ventricle and postponing pulmonic valve closure even more, so that the normal split becomes wider.
Recording provided by Jules Constant, MD.
Sound is that of fixed second heart sound (S2) splitting, ie, S1–A2–P2 at rest (“out”) and with inspiration (“in”). Splitting is fixed because the volume of flow through the right ventricle is increased throughout the respiratory cycle, eliminating the normal delay in closure of the pulmonic valve associated with inspiration.
Recording provided by Jules Constant, MD.
Sound is that of S1–S2–S3.
Recording provided by Jules Constant, MD.
Sound is that of S4–S1–S2.
Recording provided by Jules Constant, MD.
Sound is that of S4–S1–S2–S3 in rapid succession.
Recording provided by Jules Constant, MD.
A diastolic knock is a loud third heart sound (S3) caused by constrictive pericarditis.
Recording provided by Jules Constant, MD.
Sound is that of S1–A2–OS with a relatively long A2–OS interval. The opening snap (OS), most commonly caused by mitral stenosis, is thought to be caused by abrupt downward bulging (snapping) of the anterior leaflet as left ventricular pressure drops below left atrial pressure during diastole. A2–OS can be distinguished from a split S2 by dynamic maneuvers (OS intensity increases with inspiration, A2–OS interval widens with standing), a triple S2 (ie, A2–P2–OS), and a louder volume at the apex.
Recording provided by Jules Constant, MD.
S3 occurs in early diastole, when the ventricle is dilated and noncompliant. It occurs during passive diastolic ventricular filling and usually indicates serious ventricular dysfunction in adults; in children, it can be normal, sometimes persisting even to age 40 years. S3 also may be normal during pregnancy. Right ventricular S3 is heard best (sometimes only) during inspiration (because negative intrathoracic pressure augments right ventricular filling volume) with the patient supine. Left ventricular S3 is best heard during expiration (because the heart is nearer the chest wall) with the patient in the left lateral decubitus position.
S4 is produced by augmented ventricular filling, caused by atrial contraction, near the end of diastole. It is similar to S3 and heard best or only with the bell of the stethoscope. During inspiration, right ventricular S4 increases and left ventricular S4 decreases. S4 is heard much more often than S3 and indicates a lesser degree of ventricular dysfunction, usually diastolic. S4 is absent in atrial fibrillation (because the atria do not contract) but is almost always present in active myocardial ischemia or soon after myocardial infarction. Whereas S3 can be a normal finding, S4 is always abnormal.
S3, with or without S4, is usual in significant systolic left ventricular dysfunction; S4 without S3 is usual in diastolic left ventricular dysfunction.
A summation gallop occurs when S3 and S4 are present in a patient with tachycardia, which shortens diastole so that the 2 sounds merge. Loud S3 and S4 may be palpable at the apex when the patient is in the left lateral decubitus position.
A diastolic knock occurs at the same time as S3, in early diastole. It is not accompanied by S4 and is a louder, thudding sound, which indicates abrupt arrest of ventricular filling by a noncompliant, constricting pericardium.
An opening snap (OS) may occur in early diastole in mitral stenosis or, rarely, in tricuspid stenosis. Mitral opening snap is very high pitched, brief, and heard best with the diaphragm of the stethoscope. The more severe mitral stenosis is (ie, the higher the left atrial pressure), the closer the opening snap is to the pulmonic component of S2. Intensity is related to the compliance of the valve leaflets: The snap sounds loud when leaflets remain elastic, but it gradually softens and ultimately disappears as sclerosis, fibrosis, and calcification of the valve develop. Mitral opening snap, although sometimes heard at the apex, is often heard best or only at the lower left sternal border.
Approach to murmurs
Timing of the murmur in the cardiac cycle correlates with the cause (see table ); auscultatory findings correlate with specific heart valve disorders. Various maneuvers (eg, inspiration, Valsalva, handgrip, squatting, amyl nitrate inhalation) can modify cardiac physiology slightly, making differentiation of causes of heart murmur possible (see table ).
Etiology of Murmurs by Timing
Timing | Associated Disorders |
|---|---|
Mid systolic (ejection) | Outflow obstruction (aortic sclerosis, aortic stenosis, coarctation of the aorta, hypertrophic cardiomyopathy, subvalvular stenosis, supravalvular stenosis) Dilation of ascending aorta (aneurysm of aorta, aortitis, atheroma ) Dilation of pulmonary artery Increased blood flow across the aortic valve (aortic regurgitation, hyperkinetic states) Increased blood flow across the pulmonic valve (hyperkinetic states, left-to-right shunt due to atrial septal defect, ventricular septal defect) Pulmonic obstruction (infundibular stenosis, pulmonic stenosis, supravalvular pulmonary artery stenosis, branch pulmonary artery stenosis) |
Mid-late systolic | Papillary muscle dysfunction |
Holosystolic | |
Early diastolic (regurgitant) |
|
Mid diastolic | Atrial ball-valve thrombi Increased blood flow across nonstenotic mitral valve (eg, mitral regurgitation, ventricular septal defect, patent ductus arteriosus, high-output states, complete heart block) Increased blood flow across nonstenotic tricuspid valve (eg, tricuspid regurgitation, atrial septal defect, anomalous pulmonary venous return) Left or right atrial tumors Mitral stenosis (eg, due to rheumatic fever, congenital stenosis, cor triatriatum) |
Continuous | Venous hum Coronary-cameral fistula Coarctation of the aorta or pulmonary artery Severe pulmonary artery branch stenosis Anomalous left coronary artery Aortic–right ventricular or atrial fistula Bronchial collateral circulation Coronary or intercostal arteriovenous fistula Mammary souffle (venous hum from engorged breast vessels during pregnancy) Proximal coronary artery stenosis Ruptured aneurysm of sinus of Valsalva Small (restrictive) atrial septal defect with mitral stenosis |
Maneuvers That Aid in Diagnosis of Murmurs
Maneuver | Effect on Blood Flow | Effect on Heart Sounds |
|---|---|---|
Amyl nitrite | Causes intense venodilation, which reduces venous return to the right heart | Augments murmurs of hypertrophic obstructive cardiomyopathy, aortic stenosis and mitral valve prolapse Reduces murmur of mitral regurgitation |
Inspiration | Decreases intrathoracic pressure, which simultaneously increases venous flow into the right ventricle (RV) and decreases pulmonary venous flow into the left heart | Augments right heart sounds (eg, murmurs of tricuspid stenosis and regurgitation, those of pulmonic stenosis* [immediately] and regurgitation [usually]) Reduces left heart sounds |
Isometric handgrip | Increases afterload and peripheral arterial resistance | Reduces murmurs of aortic stenosis, hypertrophic obstructive cardiomyopathy, mitral valve prolapse, or papillary muscle dysfunction Augments murmurs of mitral regurgitation and aortic regurgitation and diastolic murmur of mitral stenosis |
Release of Valsalva maneuver | Increases volume of RV and left ventricle (LV) | Augments murmurs of aortic stenosis, aortic regurgitation (after 4 or 5 beats), and pulmonic regurgitation or pulmonic stenosis* (immediately) Reduces murmur of tricuspid stenosis |
Squatting | Simultaneously increases venous return to the right heart and increases afterload and peripheral resistance | Augments murmurs of aortic regurgitation, aortic stenosis, mitral regurgitation and diastolic murmur of mitral stenosis Reduces murmur of hypertrophic obstructive cardiomyopathy and mitral valve prolapse |
Valsalva maneuver | Increases intrathoracic pressure, which reduces size of LV; decreases venous return to the right heart and subsequently to the left heart | Augments murmur of hypertrophic obstructive cardiomyopathy and mitral valve prolapse Reduces murmurs of aortic stenosis, mitral regurgitation, and tricuspid stenosis |
* Patient may need to be standing for effect on pulmonic stenosis to be heard. | ||
All patients with heart murmurs are evaluated by chest radiography and electrocardiography (ECG). Echocardiography is required to confirm the diagnosis, determine severity, and track severity over time. Usually, a cardiac consultation is obtained if significant disease is suspected.
Systolic murmurs
Systolic murmurs may be normal or abnormal. They may be early, mid, or late systolic, or holosystolic (pansystolic). Systolic murmurs may be divided into ejection, regurgitant, and shunt murmurs.
Ejection murmurs are due to turbulent forward flow through narrowed or irregular valves or outflow tracts (eg, due to aortic stenosis or pulmonic stenosis). They are typically mid systolic and have a crescendo-diminuendo character that usually becomes louder and longer as flow becomes more obstructed. The greater the stenosis and turbulence, the longer the crescendo phase and the shorter the diminuendo phase.
Systolic ejection murmurs may occur without hemodynamically significant outflow tract obstruction (called innocent or functional murmurs) and thus do not necessarily indicate a disorder. In normal infants and children, flow is often mildly turbulent, producing these soft ejection murmurs. (A Still murmur is a vibratory, systolic, innocent murmur thought to be caused by vibration of the chordae tendineae of the mitral valve.) Older patients often have ejection murmurs due to valve and vessel sclerosis.
During pregnancy, many women have soft ejection murmurs at the second intercostal space to the left or right of the sternum. The murmurs occur because a physiologic increase in blood volume and cardiac output increases flow velocity through normal structures. The murmurs may be greatly exaggerated if severe anemia complicates the pregnancy. These murmurs are distinct from the venous hum sometimes caused by engorged breast vessels during pregnancy (mammary souffle).
Regurgitant murmurs represent retrograde flow (eg, due to mitral regurgitation, tricuspid regurgitation). A similar murmur can occur with a ventricular septal defect. Both are typically holosystolic and tend to be louder with high-velocity, low-volume regurgitation or shunts and softer with high-volume regurgitation or shunts.
Late systolic murmurs, which may or may not be preceded by a click, are typical of mitral valve prolapse or papillary muscle dysfunction.
Shunt murmurs may originate at the site of the shunt (eg, patent ductus arteriosus, ventricular septal defect) or result from altered hemodynamics remote from the shunt (eg, pulmonic systolic flow murmur due to an atrial septal defect with left-to-right shunt). Atrial shunt murmurs are rarely, if ever, audible.
Various maneuvers are usually required for more accurate diagnosis of timing and type of murmur (see table ).
The 6th beat is a ventricular premature beat (VPB). The 7th beat illustrates post-VPB potentiation of the murmur due to
Recording provided by Jules Constant, MD.
The murmur becomes audible only with inspiration (“in”) because inspiration decreases intrathoracic pressure, drawing m
Recording provided by Jules Constant, MD.
This holosystolic mitral regurgitation murmur maintains the same intensity throughout systole and extends from S1 to S2
Recording provided by Jules Constant, MD.
The murmur of a ventricular septal defect is similar to that of mitral regurgitation but is louder at the left lower st
Recording provided by Jules Constant, MD.
The 6th beat is a ventricular premature beat (VPB). The 7th beat illustrates post-VPB potentiation of the murmur due to increased left ventricular filling during the post-VPB compensatory pause.
Recording provided by Jules Constant, MD.
The murmur becomes audible only with inspiration (“in”) because inspiration decreases intrathoracic pressure, drawing more blood into the right ventricle and increasing right ventricular outflow.
Recording provided by Jules Constant, MD.
This holosystolic mitral regurgitation murmur maintains the same intensity throughout systole and extends from S1 to S2.
Recording provided by Jules Constant, MD.
The murmur of a ventricular septal defect is similar to that of mitral regurgitation but is louder at the left lower sternal border than at the apex.
Recording provided by Jules Constant, MD.
Diastolic murmurs
Diastolic murmurs are always abnormal; most are early or mid diastolic, but they may be late diastolic (presystolic). Early diastolic murmurs are typically due to aortic regurgitation or pulmonic regurgitation. Mid diastolic (or early to mid diastolic) murmurs are typically due to mitral stenosis or tricuspid stenosis. In a patient in sinus rhythm, a late diastolic murmur may be due to rheumatic mitral stenosis.
A mitral or tricuspid murmur due to an atrial tumor or thrombus may be evanescent and may vary with position and from one examination to the next because the position of the intracardiac mass changes.
Pearls & Pitfalls
|
Continuous murmurs
Continuous murmurs occur throughout the cardiac cycle. They are always abnormal, indicating shunt flow throughout systole and diastole, hence remaining audible through S2. They may be due to various cardiac defects (see table ). Some defects produce a thrill; many are associated with signs of right or left ventricular hypertrophy. As pulmonary artery resistance increases in shunt lesions, the diastolic component gradually decreases. When pulmonary and systemic resistance equalize, the murmur may disappear.
Patent ductus arteriosus murmurs are loudest at the second intercostal space just below the medial end of the left clavicle. Aortopulmonary window murmurs are central and heard at the third intercostal space level. Murmurs of systemic arteriovenous fistulas are best heard directly over the lesions; those of pulmonic arteriovenous fistulas and pulmonary artery branch stenosis are more diffuse and heard throughout the chest.
When circulation is increased, as occurs during pregnancy, anemia, and hyperthyroidism, a continuous venous hum is often heard in the right supraclavicular fossa; this venous hum also occurs normally in children. The sound generated by increased flow in a dilated internal mammary artery (mammary souffle), may be mistaken for a continuous cardiac murmur. Mammary souffle is typically heard best over the breast at the level of the right and/or left second or third intercostal space and, although often classified as continuous, is usually louder during systole.
Pericardial friction rub
A pericardial friction rub is caused by movement of inflammatory adhesions between visceral and parietal pericardial layers. It is a high-pitched or squeaking sound; it may be systolic, diastolic and systolic, or triphasic (when atrial contraction accentuates the diastolic component during late diastole). The rub sounds like pieces of leather squeaking as they are rubbed together. Rubs are best heard with the patient leaning forward or on hands and knees with breath held in expiration.
Reference
1. Fang JC, O'Gara PT: History and Physical Examination: An Evidence-Based Approach. In Libby P, Bonoow RO, Mann DL, et al (eds): Braunwald's Heart Disease: A Textbook of Cardiovascular Medicine, 12th ed. Philadelphia, Elsevier, 2022, pp 123-140.





