



Infants whose weight is > the 90th percentile for gestational age are classified as large for gestational age. Macrosomia is birthweight > 4000 g in a term infant. The predominant cause is maternal diabetes. Complications include birth trauma, hypoglycemia, hyperviscosity, and hyperbilirubinemia. Treatment is directed at managing birth and postnatal complications, which are more common among neonates who are large for gestational age.
Gestational age is loosely defined as the number of weeks between the first day of the mother's last normal menstrual period and the day of delivery. More accurately, the gestational age is the difference between 14 days before the date of conception and the date of delivery. Gestational age is not the actual embryologic age of the fetus, but it is the universal standard among obstetricians and neonatologists for discussing fetal maturation.
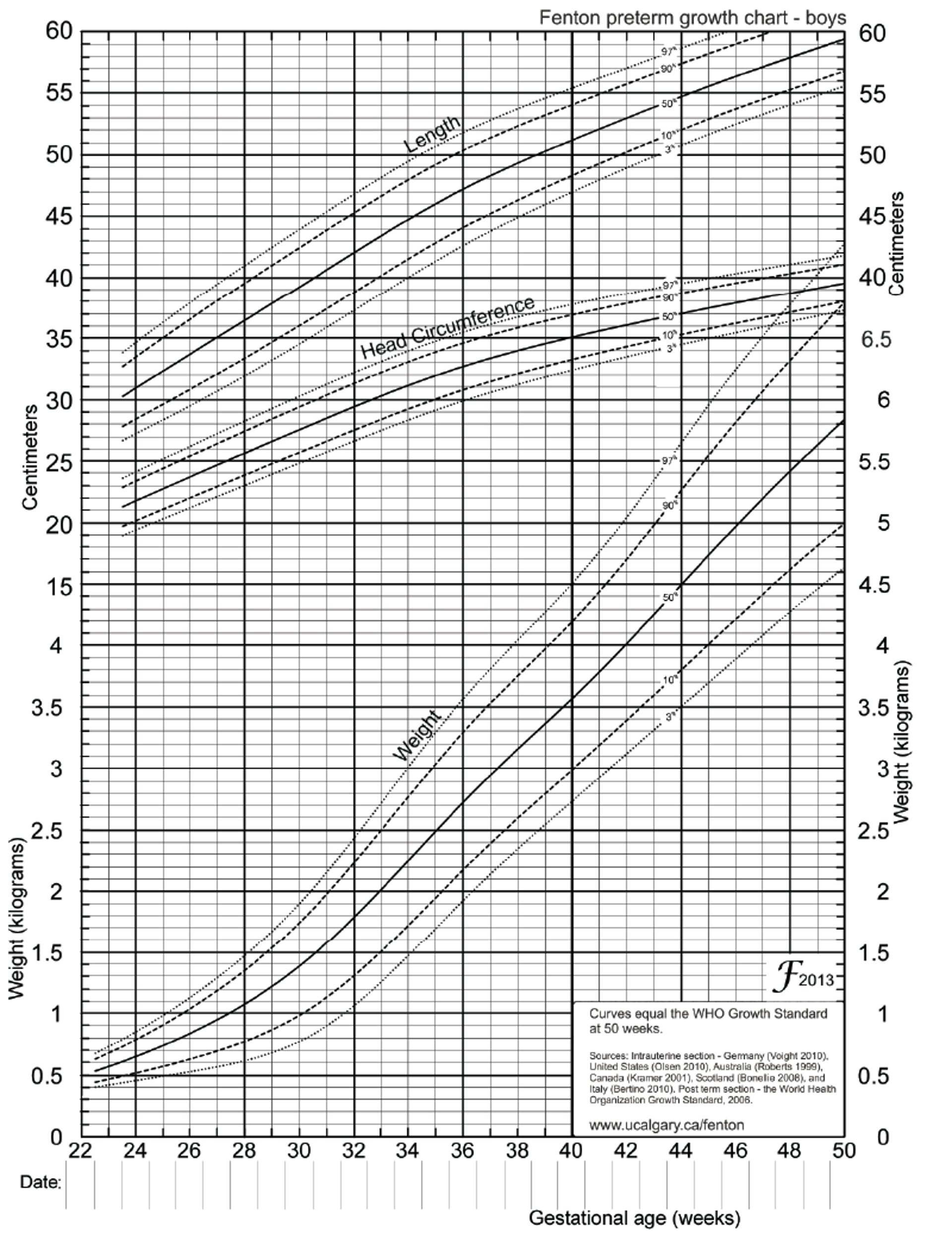
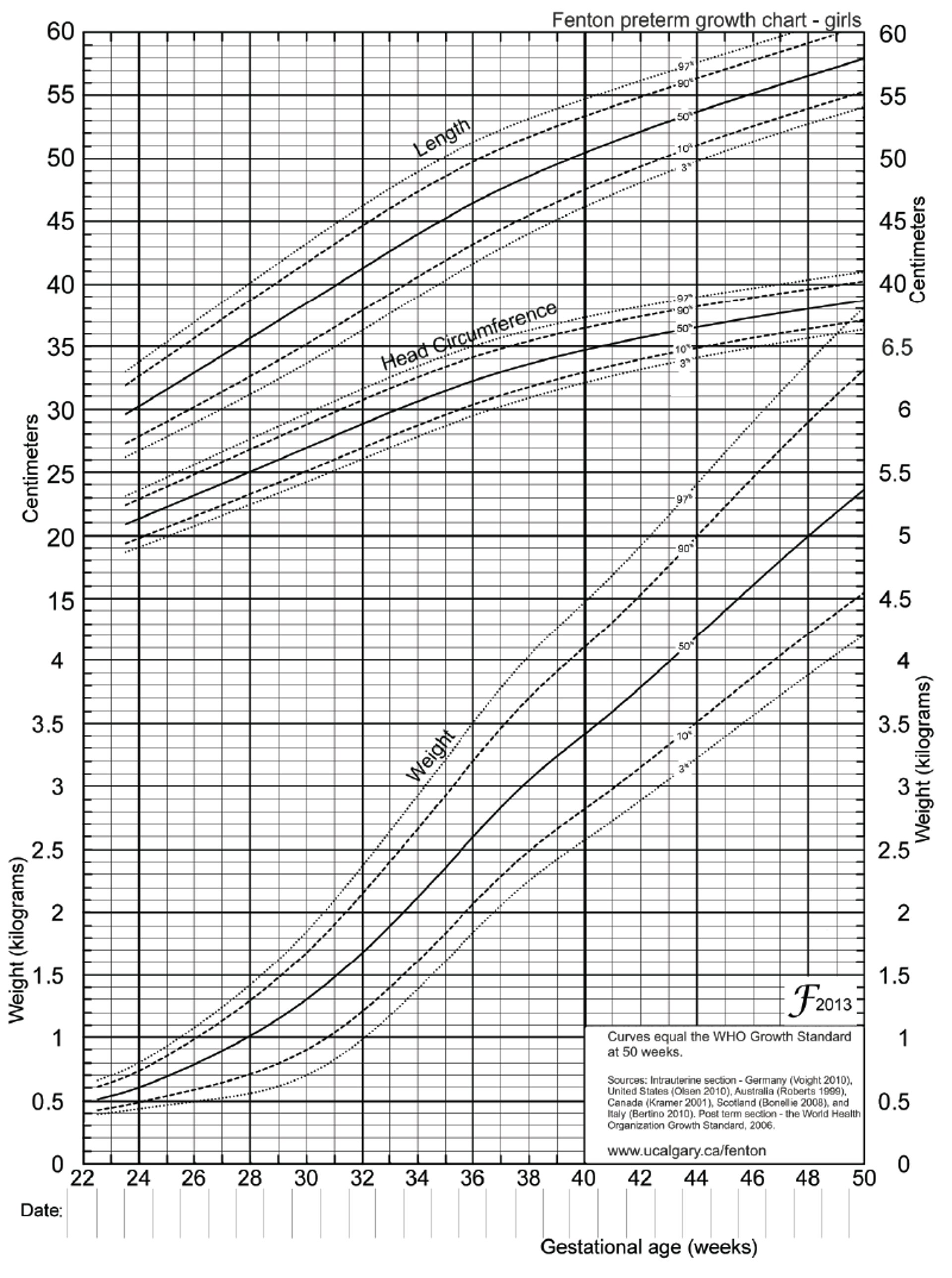
The Fenton growth charts provide a more precise assessment of growth vs gestational age (see figures and ).
Fenton Growth Chart for Preterm Boys
Fenton T, Kim J: A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatrics 13:59, 2013. doi: 10.1186/1471-2431-13-59; used with permission. |

Fenton Growth Chart for Preterm Girls
Fenton T, Kim J: A systematic review and meta-analysis to revise the Fenton growth chart for preterm infants. BMC Pediatrics 13:59, 2013. doi: 10.1186/1471-2431-13-59; used with permission. |

Etiology of LGA Infant
Other than genetically determined size, maternal diabetes mellitus is the major cause of large-for-gestational-age (LGA) infants. The large size results from the anabolic effects of high fetal insulin levels produced in response to excessive maternal blood glucose during gestation and sometimes increased caloric intake by the mother to compensate for glucose lost in urine. The less well controlled the mother’s diabetes during pregnancy, the larger is the size of the fetus. Another contributing factor is maternal obesity.
Rare causes of macrosomia are Beckwith-Wiedemann syndrome (characterized by macrosomia, omphalocele, macroglossia, and hypoglycemia) and Sotos, Marshall, and Weaver syndromes.
Symptoms, Signs, and Treatment of LGA Infant
LGA infants are large and plethoric. The 5-minute may be low. These infants may be listless and limp and feed poorly.
Delivery complications can occur in any LGA infant. Congenital anomalies and some metabolic and cardiac complications are specific to LGA infants of mothers with diabetes.
Delivery complications
Because of the infant’s large size, vaginal delivery may be difficult and occasionally results in birth injury, particularly including
Perinatal asphyxia
Other complications occur when weight is > 4000 g. There is a proportional increase in morbidity and mortality because of the following:
Respiratory distress (and need for ventilatory assistance)
Infants of mothers with diabetes
Infants of mothers with diabetes are at risk of
Certain congenital anomalies
Hypoglycemia is very likely in the first few hours after delivery because of the state of hyperinsulinism and the sudden termination of maternal glucose when the umbilical cord is cut. Neonatal hypoglycemia can be decreased by close prenatal control of the mother’s diabetes and early, frequent feedings of any neonate at risk of developing hypoglycemia (1). Blood glucose levels should be closely monitored by bedside testing from birth through at least the first 24 hours (2).
Treatment of hypoglycemia can range from enteral feeding orally or via nasogastric tube to IV administration of dextrose-containing fluids. Oral treatment with 40% glucose gel may prevent the need to separate the neonate from the mother for IV placement, but if hypoglycemia is persistent, parenteral dextrose-containing fluids are given IV. There is also evidence that prophylactic use of oral glucose gel may prevent hypoglycemia in at-risk neonates (3). More evidence is needed about the effects of oral gel on long-term neurologic disability compared to other therapies for hypoglycemia (4).
Hypocalcemia and hypomagnesemia may occur but are usually transient and asymptomatic. Good prenatal glycemic control decreases the risk of neonatal hypocalcemia. Hypocalcemia typically does not require treatment unless there are clinical signs of it (eg, jitteriness, seizures, apnea) or total serum calcium levels are < 7 mg/dL (< 1.75 mmol/L) or ionized calcium levels are < 4 mg/dL (< 1 mmol/L) in term infants. Treatment should be based on ionized calcium levels because these levels more accurately reflect available calcium. Treatment is usually given with IV supplementation of calcium gluconate. Hypomagnesemia can interfere with the secretion of parathyroid hormone, so hypocalcemia may not respond to treatment until the magnesium level is corrected.
Polycythemia is slightly more common among infants of mothers with diabetes. Elevated insulin levels increase fetal metabolism and thus oxygen consumption. If the placenta is unable to meet the increased oxygen demand, fetal hypoxemia occurs, triggering an increase in erythropoietin and thus hematocrit.
Hyperbilirubinemia occurs for several reasons. Infants of mothers with diabetes often have decreased tolerance for oral feedings (particularly when they are preterm) in the earliest days of life, which increases the enterohepatic circulation of bilirubin. Also, if polycythemia is present, the bilirubin load increases.
Respiratory distress syndrome (RDS) may occur because elevated insulin levels decrease surfactant production; pulmonary maturation may thus be delayed until late in gestation. RDS may develop even if the infant is delivered late preterm or term. Treatment of respiratory distress syndrome is discussed elsewhere.
Transient tachypnea of the newborn is 2 to 3 times more likely in infants of mothers with diabetes because of the delay in fetal lung fluid clearance.
Congenital anomalies are more likely in infants of mothers with diabetes because maternal hyperglycemia at the time of organogenesis is detrimental. Specific anomalies include
Congenital heart disease (hypertrophic cardiomyopathy, ventricular septal defect, transposition of the great arteries, and aortic stenosis)
Caudal regression syndrome
Small left colon syndrome
Persistently elevated insulin levels can also lead to increased deposition of glycogen and fat into cardiomyocytes. This deposition can cause transient hypertrophic cardiomyopathy, predominantly of the septum.
References
1. Committee on Fetus and Newborn, Adamkin DH. Postnatal glucose homeostasis in late-preterm and term infants. Pediatrics. 2011;127(3):575-579. doi:10.1542/peds.2010-3851
2. Thornton PS, Stanley CA, De Leon DD, et al. Recommendations from the Pediatric Endocrine Society for Evaluation and Management of Persistent Hypoglycemia in Neonates, Infants, and Children. J Pediatr. 2015;167(2):238-245. doi:10.1016/j.jpeds.2015.03.057
3. Devarapalli V, Niven M, Canonigo J, et al. Prophylactic dextrose gel use in newborns at risk for hypoglycemia. J Perinatol. 2024;44(11):1640-1646. doi:10.1038/s41372-024-02133-9
4. Edwards T, Liu G, Battin M, et al. Oral dextrose gel for the treatment of hypoglycaemia in newborn infants. Cochrane Database Syst Rev. 2022;3(3):CD011027. doi:10.1002/14651858.CD011027.pub3
Key Points
Maternal diabetes mellitus is the main cause of large-for-gestational-age infants.
Large size itself increases risk of birth injury (eg, clavicle or extremity long bone fracture) and perinatal asphyxia.
Infants of mothers with diabetes also may have metabolic complications immediately after delivery, including hypoglycemia, hypocalcemia, and polycythemia.
Infants of mothers with diabetes are also at risk of respiratory distress syndrome and congenital anomalies.
Good control of maternal glucose levels minimizes risk of complications.
Drug Information for the Topic





