





Ulcerative colitis is a chronic inflammatory bowel disease in which the large intestine (colon) becomes inflamed and ulcerated (pitted or eroded), leading to flare-ups (bouts or attacks) of bloody diarrhea, abdominal cramps, and fever. The long-term risk of colon cancer is higher than in people who do not have ulcerative colitis.
The exact cause of this disease is not known.
Typical symptoms during flare-ups include abdominal cramps, an urge to move the bowels, and diarrhea (typically bloody).
The diagnosis is based on a sigmoidoscopy or sometimes a colonoscopy.
People who have had ulcerative colitis for a long time are at increased risk for colon cancer.
Treatment is aimed at controlling the inflammation, reducing symptoms, and replacing any lost fluids and nutrients.
(See also Overview of Inflammatory Bowel Disease (IBD).)
Locating the Large Intestine (Colon)

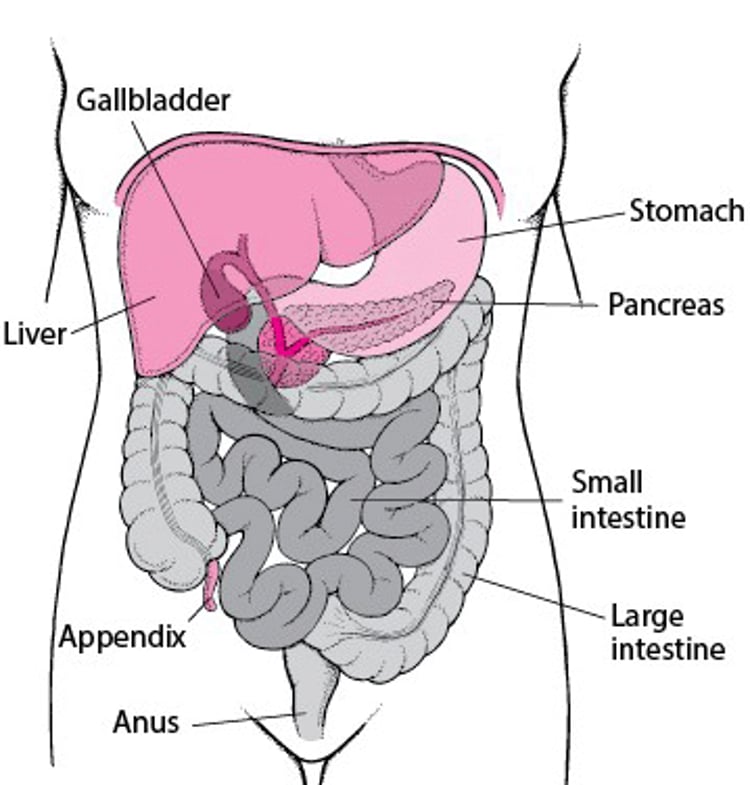

Ulcerative colitis usually starts in the rectum (ulcerative proctitis). It may stay confined to the rectum or over time extend to involve the entire colon. In some people, most of the large intestine is affected at once.
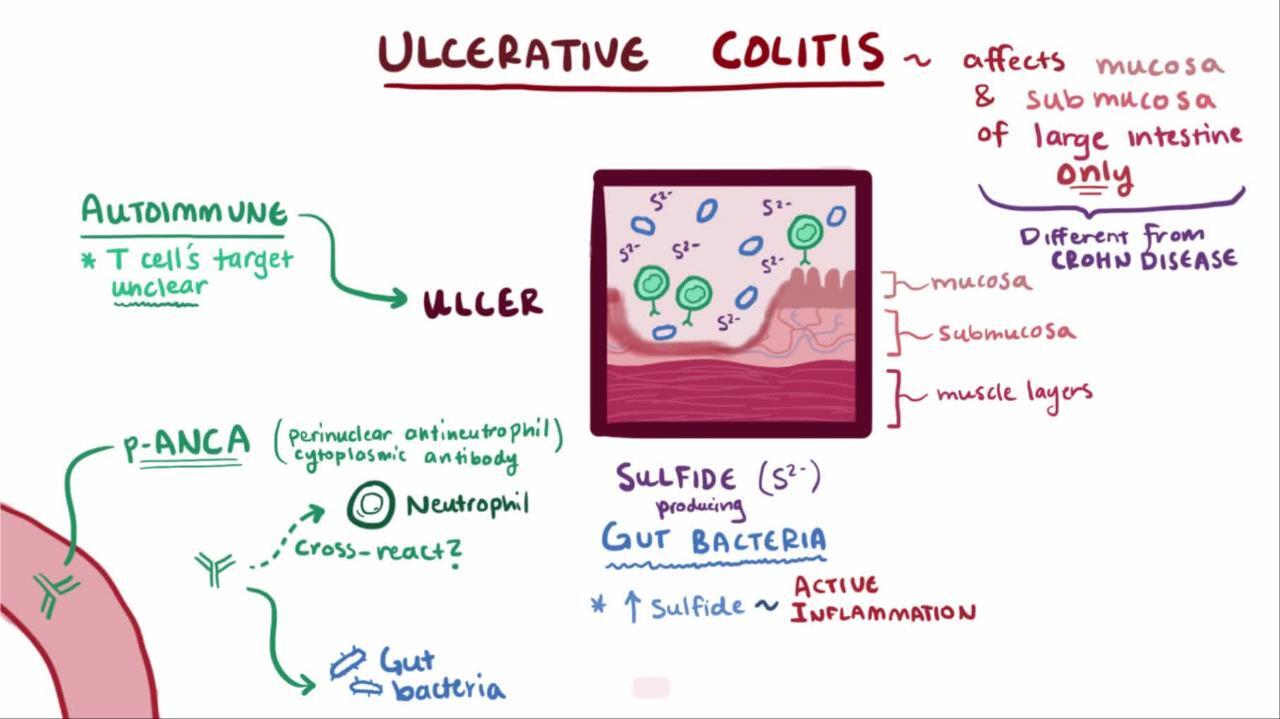
Ulcerative colitis usually does not affect the full thickness of the wall of the large intestine and hardly ever affects the small intestine. The affected parts of the intestine have shallow ulcers (sores). Unlike Crohn disease, ulcerative colitis does not cause fistulas or abscesses.
The cause of ulcerative colitis is not known for certain, but heredity and an overactive immune response in the intestine seem to be contributing factors. Cigarette smoking, which seems to contribute to the development and periodic flare-ups of Crohn disease, seems to decrease the risk of ulcerative colitis. (However, smoking in order to reduce the risk of ulcerative colitis is not advised in light of the many health problems that smoking can cause.)

Symptoms of Ulcerative Colitis
The symptoms of ulcerative colitis occur in flare-ups with bloody diarrhea. A flare-up usually begins gradually, and the person has an urgency to have a bowel movement (defecate), mild cramps in the lower abdomen, and visible blood and mucus in the stool. Sometimes, a flare-up is sudden and severe, causing violent diarrhea that typically contains mucus and blood, high fever, abdominal pain, and occasionally peritonitis (inflammation of the lining of the abdominal cavity, causing severe pain across the entire abdomen). During such flare-ups, the person is profoundly ill. A flare-up can last days or weeks and can recur at any time.
When the disease is limited to the rectum and the sigmoid colon, the stool may be normal or hard and dry. However, mucus containing large numbers of red and white blood cells is discharged from the rectum during or between bowel movements. People may or may not have mild general symptoms of illness, such as fever.
If the disease extends farther up the large intestine, the stool is looser, and the person may have more than 10 bowel movements a day. Often, the person has severe abdominal cramps and distressing, painful spasms that accompany the urge to defecate. There is no relief at night. The stool may be watery or contain mucus. Frequently, the stool consists almost entirely of blood and pus. The person also may have a fever and a poor appetite and may lose weight.
Complications of ulcerative colitis
The main serious complications of ulcerative colitis include
Bleeding
Fulminant colitis (toxic colitis)
Colon cancer
Bleeding, the most common complication, often causes iron deficiency anemia.
Fulminant colitis (also called toxic colitis) is a particularly severe complication. In some people who have ulcerative colitis, a rapidly progressing first attack becomes very severe, with massive bleeding, rupture (perforation) of the colon, or widespread infection. Damage to the nerves and muscles of the bowel wall causes ileus (a condition in which the normal contractile movements of the intestinal wall temporarily stop), and thus the intestinal contents are not propelled along their way. Abdominal expansion (distention) develops.
As fulminant colitis worsens, the large intestine loses muscle tone and within days—or even hours—it starts to expand (a condition sometimes referred to as toxic megacolon). This complication may cause a high fever and abdominal pain. Sometimes there is a perforation of the large intestine and the person develops peritonitis. X-rays or other imaging tests of the abdomen may show expansion of the bowel and the presence of gas inside the wall of the paralyzed sections of intestine.
Colon cancer starts to become more common by about 7 years from when ulcerative colitis started in people with extensive colitis. The risk of colon cancer is highest when the entire large intestine is affected and increases the longer the person has had ulcerative colitis. However, people who have both inflammatory bowel disease and inflammation of the bile ducts (primary sclerosing cholangitis) are at a higher risk of colon cancer starting from the time when the colitis is diagnosed.
Colonoscopy (examination of the large intestine using a flexible viewing tube) every 1 to 2 years is advised for people who have had ulcerative colitis for more than 8 to 10 years or who have primary sclerosing cholangitis. During colonoscopy, tissue samples are taken from areas throughout the large intestine for examination under a microscope to detect the early warning signs of cancer (dysplasia). This removal and examination of tissue is called a biopsy. In a newer type of colonoscopy called chromoendoscopy, dyes are inserted into the colon during colonoscopy to highlight cancerous (malignant) and precancerous areas and may better help doctors identify areas for biopsy.
Other complications can occur, as in Crohn disease. When ulcerative colitis causes a flare-up of gastrointestinal symptoms, people also may have the following:
Inflammation of the joints (arthritis)
Inflammation of the whites of the eyes (episcleritis)
Inflamed skin nodules (erythema nodosum)
When ulcerative colitis is not causing a flare-up of gastrointestinal symptoms, people still may have complications that occur entirely without relation to the bowel disease such as the following:
Dusky purple skin sores that may contain pus (pyoderma gangrenosum)
Inflammation of the spine
Inflammation of the pelvic joints (sacroiliitis)
Inflammation of the inside of the eye (uveitis)
Although people with ulcerative colitis commonly have minor liver dysfunction, only about 1 to 3% have symptoms of liver disease, which vary from mild to severe. Severe liver disease can include inflammation of the liver (chronic active hepatitis), inflammation of the bile ducts (primary sclerosing cholangitis), which narrow and eventually close, and replacement of functional liver tissue with scar tissue (cirrhosis). Inflammation of the bile ducts may appear many years before any intestinal symptoms of ulcerative colitis. The inflammation greatly increases the risk of cancer of the bile ducts and also seems to be associated with a sharp increase in the risk of colon cancer.
Diagnosis of Ulcerative Colitis
Stool tests
Colonoscopy or sigmoidoscopy with biopsy
Blood tests
Sometimes imaging tests
Doctors suspect ulcerative colitis in a person with recurring bloody diarrhea accompanied by cramps and a strong urge to defecate, particularly if the person has other complications, such as arthritis or liver problems, and a history of similar attacks.
Doctors examine the stool to look for parasites, exclude bacterial infections, and assess inflammation.
Colonoscopy (an examination of the colon using a flexible viewing tube) confirms the diagnosis of ulcerative colitis. Flexible sigmoidoscopy, a more limited and safer examination, is an alternative for people with higher risk of intestinal perforation. This procedure permits a doctor to directly observe the severity of the inflammation, take samples of mucus or stool for culture, and remove tissue samples of affected areas for examination under a microscope (called a biopsy). Even during symptom-free intervals, the intestine rarely appears entirely normal, and tissue samples removed for examination under a microscope usually show chronic inflammation.
Blood tests do not confirm the diagnosis of ulcerative colitis but may reveal that the person has anemia, increased numbers of white blood cells (occurs with inflammation), a low level of the protein albumin, and an elevated erythrocyte sedimentation rate (ESR) or C-reactive protein level, which also indicate active inflammation. A doctor may also do liver tests.
X-rays of the abdomen taken after barium is given by enema (called a barium enema) may indicate the severity and extent of the disease but are not done when the disease is active, such as during a flare-up, because of the risk of causing a perforation. Other x-rays of the abdomen may also be taken.
Doctors may look for other causes of colitis, including ischemic colitis in the elderly, contraceptive-induced colitis in those taking contraceptives, and immune-mediated colitis in those taking certain medications called immune checkpoint inhibitors.
Recurring or severe symptoms of ulcerative colitis
Doctors examine people when their typical symptoms return, but they do not always do tests. If symptoms have been more frequent or longer-lasting than usual, doctors may do sigmoidoscopy or colonoscopy and a blood count. Doctors may do other tests to look for infection or parasites.
Treatment of Ulcerative Colitis
Dietary management and loperamide
Aminosalicylates
Steroids
Immunomodulating medications
Biologic and related agents
Small-molecule agents
Sometimes surgery
Ulcerative colitis treatment aims to control the inflammation, reduce symptoms, and replace any lost fluids and nutrients. Specific treatment depends on the severity of people's symptoms.
General approach to ulcerative colitis treatment
Usually, if the large intestine is swollen, people should eat a low-fiber diet (in particular, avoiding foods such as nuts, corn hulls, raw fruits, and vegetables) to reduce injury to the inflamed lining of the large intestine. However, a high-fiber diet should be resumed once the IBD flare resolves.
A diet free of dairy products may decrease symptoms and is worth trying but does not need to be continued if no benefit is noted.
All people who have ulcerative colitis should take calcium and vitamin D supplements. Iron supplements may offset anemia caused by ongoing blood loss in the stool.
Small doses of loperamide are taken for relatively mild diarrhea. For more intense diarrhea, higher doses of loperamide may be needed. In severe cases, however, a doctor must closely monitor the person taking these antidiarrheal medications because of the risk of fulminant colitis.
Routine health maintenance measures, particularly vaccinations and cancer screening, are important.
Did You Know...
|
For people with mild symptoms and disease confined to the left side of the colon, mesalamine enemas or suppositories are usually used first. In people for whom this treatment is not effective, other options include oral mesalamine (5-ASA), tacrolimus or beclomethasone suppositories, or oral budesonide MMX.
For people with moderate or extensive disease, biologic agents (infliximab, adalimumab, golimumab, guselkumab, risankizumab, mirikizumab, ustekinumab, vedolizumab) sometimes with an immunomodulator (azathioprine or 6-mercaptopurine) are used. Other options include high-dose steroids or small molecule medications (tofacitinib, upadacitinib, ozanimod, or etrasimod).
People with severe disease, which can include more than 6 bowel movements daily, elevated heart rate, fever, or severe abdominal pain, are cared for in the hospital and typically receive biologic agents and/or high-dose IV steroids. They may need IV fluids or blood transfusions. They should also receive treatment to prevent blood clots. Combinations of medications, or other medications that suppress the immune system (cyclosporine, tacrolimus) may be used in patients who do not get better with the initial treatment. Surgery is sometimes needed.
For people with life-threatening (fulminant) colitis (more than 10 stools per day with continuous blood, enlargement of the colon with fever, elevated heart rate, and laboratory tests indicating inflammation), hospitalization is required. People may not eat or drink and receive IV fluids and electrolytes, antibiotics, and IV treatment such as steroids, cyclosporine, or infliximab.
Aminosalicylates
Aminosalicylates are medications used to reduce the inflammation of ulcerative colitis and to prevent flare-ups of symptoms. Medications such as sulfasalazine, olsalazine, mesalamine, and balsalazide are types of aminosalicylates. For ulcerative colitis, mesalamine by enema or suppository is most often used. Whether given orally or rectally, these medications are at best moderately effective for treating mild or moderately active disease, but they are more effective for preventing symptoms from reappearing (maintaining remission).
Steroids
People with moderately severe disease usually take steroids (such as prednisone) in fairly high doses, which frequently induces a dramatic remission. After steroids control the inflammation of ulcerative colitis, sulfasalazine, olsalazine or mesalamine, or an immunomodulating medication, a biologic agent, or tofacitinib or ozanimod is often given to maintain the improvement. Gradually, the prednisone dosage is decreased, and ultimately the prednisone is discontinued.
Budesonide is another steroid that may be used in a long-acting oral form for ulcerative colitis
Long-term steroid treatment almost always causes side effects (see sidebar ).
If the disease becomes severe, the person is hospitalized, and steroids and fluids are given by vein (intravenously).
Immunomodulating medications
Immunomodulating medications modify the action of the body's immune system, decreasing its activity. Medications such as azathioprine, and mercaptopurine have been used to maintain remissions in people with ulcerative colitis who would otherwise need long-term steroid treatment. These medications inhibit the function of T cells, which are an important component of the immune system. However, these medications are slow to act, and a benefit may not be seen for 1 to 3 months. They also have potentially serious side effects that require close monitoring by the doctor.
Cyclosporine has been given to some people who have severe flare-ups and have not responded to steroids. Most of these people respond initially to the cyclosporine, but some may still ultimately require surgery.
Tacrolimus is given by mouth. This medication has been given as short-term treatment to people whose ulcerative colitis is difficult to manage while they begin treatment with other medications. Tacrolimus may help maintain remission.
Biologic agents
Biologic agents are medicines that are created by living organisms.
Before starting treatment with other biologic agents, people should be tested for tuberculosis, hepatitis B infection, and hepatitis C infection.
Infliximab, which is derived from monoclonal antibodies to tumor necrosis factor (called a tumor necrosis factor inhibitor or TNF inhibitor) and given intravenously, is beneficial for some people with ulcerative colitis. This medication may be given to people who do not respond to steroids or who develop symptoms whenever steroid doses are lowered, despite the optimal use of other immunomodulating medications. Infliximab, adalimumab, and golimumab are beneficial for people whose ulcerative colitis is difficult to treat or for people who depend on steroids.
Side effects that may occur with infliximab include worsening of an existing uncontrolled bacterial infection, reactivation of tuberculosis or hepatitis B, and an increase in the risk of some types of cancer. Some people have reactions such as fever, chills, nausea, headache, itching, or rash during the infusion (called infusion reactions). Before starting treatment with infliximab or other TNF inhibitors such as adalimumab and golimumab, people must be tested for tuberculosis and hepatitis B infections.
Vedolizumab is a medication for people who have (1) moderate to severe ulcerative colitis that has not responded to TNF inhibitors or other immunomodulating medications or who (2) are unable to tolerate these medications. The most serious side effect it causes is increased susceptibility to infection. Vedolizumab has a theoretical risk of a serious brain infection called progressive multifocal leukoencephalopathy (PML) because this infection has been reported with the use of a related medication called natalizumab.
Ustekinumab is another kind of biologic agent given to people who have moderate to severe ulcerative colitis that has not responded to TNF inhibitors or other immunomodulating medications or who are unable to tolerate these medications. The first dose is given by vein and then by injections under the skin every 8 weeks. Side effects include injection-site reactions (pain, redness, swelling), cold-like symptoms, chills, and headache.
Adalimumab, golimumab, guselkumab, risankizumab, mirikizumab, (other biologic agents) are prescribed for moderate to severe Crohn disease or ulcerative colitis. For some of these medications, liver tests are checked before and during treatment to monitor for liver damage. Doctors also monitor the person for other symptoms, including injection site reactions, skin rashes, and viral infections.
Side Effects of Selected Medications for Ulcerative Colitis
Medication | Some Side Effects | Comments |
|---|---|---|
Aminosalicylates | ||
| Common: Nausea, headache, dizziness, fatigue, fever, rash, and, in men, reversible infertility Uncommon: Inflammation of the liver (hepatitis), pancreas (pancreatitis), or lung (pneumonitis) and hemolytic anemia | Abdominal pain, dizziness, and fatigue are related to dose. Hepatitis and pancreatitis are unrelated to dose. |
| Common: Fever and rash Uncommon: Pancreatitis, inflammation of the pericardium (pericarditis), and pneumonitis For olsalazine: Watery diarrhea | Most side effects seen with sulfasalazine may occur with any of the other aminosalicylates but much less frequently. |
Steroids | ||
Prednisone | Diabetes mellitus, high blood pressure, cataracts, osteoporosis (decreased bone density), thinning of skin, mental problems, acute psychosis, mood swings, infections, acne, excessive body hair (hirsutism), menstrual irregularities, gastritis, and peptic ulcer disease | Diabetes and high blood pressure are more likely to occur in people who have other risk factors. |
Budesonide | Diabetes mellitus, high blood pressure, cataracts, and osteoporosis | Budesonide causes the same side effects as prednisone but to a lesser degree. |
Hydrocortisone (enema or foam) | Some of the medication is absorbed by the body, but even with long-term use, few people have serious side effects (unlike with steroids such as prednisone). | Hydrocortisone enema or foam is mainly for ulcerative colitis affecting the rectum or large intestine near the rectum. |
Immunomodulators | ||
| Anorexia, nausea, vomiting, general feeling of illness, infection, cancer, allergic reactions, pancreatitis, low white blood cell count, bone marrow suppression, and liver dysfunction | Side effects that are usually dose dependent include bone marrow suppression and liver dysfunction. Interval blood monitoring is required. |
Cyclosporine | High blood pressure, nausea, vomiting, diarrhea, kidney failure, tremors, infections, seizures, neuropathy, and development of lymphomas (cancers of the lymphatic system) | Side effects become more likely with long-term use. |
Tacrolimus | Similar to cyclosporine | This medication is closely related to cyclosporine and shares a number of its side effects. |
Biologic and related agents | ||
Infliximab | Infusion reactions, infections, cancer, abdominal pain, liver dysfunction, and low white blood cell count | Infusion reactions are potentially immediate side effects that occur during the infusion (such as fever, chills, nausea, headache, itching, rash, hives, decreased blood pressure, or difficulty breathing). People should be screened for tuberculosis and hepatitis B before initiating treatment. |
Adalimumab | Pain or itching at the injection site (hypersensitivity reactions), headache, infections, and cancer | Side effects are similar to those of infliximab except adalimumab is given under the skin (subcutaneously) and so does not cause infusion reactions. Other hypersensitivity reactions that occur at the injection site include rash and hives. More severe hypersensitivity reactions are possible. |
Golimumab | When given subcutaneously, pain or itching at the injection site (hypersensitivity reactions), infections, and cancer | Side effects are similar to those of infliximab. When given subcutaneously, this medication does not cause infusion reactions. Other hypersensitivity reactions that occur at the injection site include rash and hives. More severe hypersensitivity reactions are possible. |
Vedolizumab | Infections, hypersensitivity reactions, common colds | Very rare risk of progressive multifocal leukoencephalopathy (PML). |
Ustekinumab | Injection site reactions (pain, redness, swelling), cold-like symptoms, chills, headache, tired feeling, diarrhea, lower back pain, painful urination, or rash or itching | This medication might increase the risk of cancer. Squamous cell carcinoma, a type of skin cancer, may occur. A disorder that causes the brain to swell (reversible posterior leukoencephalopathy syndrome) may occur. |
Mirikizumab | Increased risk of upper respiratory infections and cold sores, injection site reactions (pain, redness, or swelling), headache, joint pain | People should be screened for tuberculosis before treatment. Liver enzymes and bilirubin are checked before and during treatment. All age-appropriate vaccinations should be completed before treatment. All live vaccines must be avoided during treatment. |
Risankizumab | Infections, headache, fatigue, common cold | Most of these side effects will improve within a couple of weeks |
Guselkumab | Hypersensitivity reaction, increased risk of upper respiratory infection | People should be screened for tuberculosis, hepatitis B, and hepatitis C before treatment. Liver enzymes and bilirubin are checked before and during treatment. All age-appropriate vaccinations must be completed before treatment. All live vaccines must be avoided during treatment. This medication should not be used in uncontrolled infections (including tuberculosis, HIV, or hepatitis B) without prophylaxis. |
Small-molecule agents | ||
Tofacitinib | Increased risk of elevated cholesterol levels, headache, herpes zoster (shingles) infection, and other infections Other rare side effects include increased risk of blood clot, heart attack, and stroke. | People should be screened for tuberculosis before and during treatment. |
Upadacitinib | Increased risk of elevated cholesterol levels, headache, herpes zoster (shingles) infection, and other infections Other rare side effects include increased risk of blood clot, heart attack, and stroke. | People should be screened for tuberculosis before and during treatment. |
Ozanimod | Upper respiratory tract infections, headache, liver inflammation | People should be screened for tuberculosis before starting treatment. This medication should not be taken by people who take a monoamine oxidase inhibitor (MAOI—such as selegiline, phenelzine, and linezolid). |
Etrasimod | Increased risk of infections, decreased white blood cell count | This medication is not for use in patients with history of heart attack or unstable angina, heart failure, stroke, and some heart rhythm problems. |
Small-molecule agents
Tofacitinib is a medication given by mouth twice a day for adults with moderate to severe ulcerative colitis. This medication is a Janus kinase (JAK) inhibitor. It is not actually a biologic agent because it is created by chemical processes rather than by living organisms. However, it shares many characteristics with biologic agents, including many of their side effects. Tofacitinib interferes with the communication between cells that coordinate inflammation by inhibiting an enzyme (Janus kinase, or JAK). Serious side effects include increased susceptibility to infection, blood clot (such as in deep vein thrombosis or pulmonary embolism), heart attack, and stroke.
Upadacitinib is a medication given by mouth once a day for adults with moderate to severe ulcerative colitis. It is also a JAK inhibitor (described above). In general, the side effects are similar to those of other JAK inhibitors (such as tofacitinib). JAK inhibitors may cause blood disorders, in which case the medication is discontinued. They are also given with caution to people who are at risk of certain gastrointestinal disorders, and they should be avoided in people with an increased risk of cardiovascular events such as heart attack, stroke, or even death.
Ozanimod is a medication given by mouth for adults with moderate to severe active ulcerative colitis. This medication should not be used by people who have had a heart attack, chest pain (unstable angina), stroke or mini-stroke (transient ischemic attack or TIA), or certain types of heart failure in the last 6 months. This medication also should not be taken by people who have or have had a history of certain types of an irregular or abnormal heartbeat (arrhythmia) that is not corrected by a pacemaker, by people with severe untreated sleep apnea, or by people who take a monoamine oxidase inhibitor (MAOI—such as selegiline, phenelzine, and linezolid). Ozanimod can increase the risk of infections, slow the heart rate, lower the number of white blood cells, and cause liver damage.
Etrasimod works by modifying the immune response, thus reducing the movement of white blood cells into inflamed tissue. This is the mechanism by which the medication controls inflammation in the gastrointestinal tract. However, this mechanism can also suppress the immune system enough to increase the risk of infections, some of which can be serious. People with certain cardiovascular disorders (for example, myocardial infarction, stroke, and heart failure) should not take etrasimod.
Severity of symptoms
People with ulcerative proctitis, or colitis that affects only the part of the colon near the rectum, are given mesalamine enemas. Steroid and budesonide enemas are given to people who are not helped by or cannot tolerate mesalamine.
People with moderate or extensive disease are given mesalamine by mouth in addition to mesalamine enemas. People with severe symptoms and those who still have symptoms while using mesalamine usually take oral steroids such as prednisone. Prednisone in fairly high doses frequently induces a dramatic remission. After prednisone controls the inflammation of ulcerative colitis, sulfasalazine, olsalazine, or mesalamine often is given to maintain the improvement. Gradually, the prednisone dosage is decreased, and ultimately the prednisone is discontinued because prolonged steroid treatment almost always causes side effects.
People whose symptoms return when prednisone is decreased are sometimes given an immunomodulating medication (azathioprine or mercaptopurine). Additionally, some people benefit from infliximab, adalimumab, vedolizumab, golimumab, ustekinumab, tofacitinib, or ozanimod.
People with severe colitis are hospitalized, and high-dose steroids and fluids are given intravenously. Doctors may continue to give mesalamine. People with heavy rectal bleeding may require blood transfusions. People who do not respond to these treatments within 3 to 7 days may be given intravenous infliximab, vedolizumab, or cyclosporine or may need surgery to remove their colon. People who have severe or difficult-to-treat colitis but who do not need to be hospitalized may be given tacrolimus.
Fulminant colitis (toxic colitis)
People whose disease occurs suddenly, rapidly, and with great pain or who may have toxic colitis are hospitalized. All antidiarrheal medications are stopped, no food or medications are given by mouth, and doctors pass a tube through the nose and into the stomach or small intestine to remove contents from the stomach or small intestine. People are given intravenous fluids and electrolytes and high-dose intravenous steroids or cyclosporine. Doctors also give antibiotics. People may be given infliximab.
People are monitored closely for signs of infection or a perforation. People whose condition does not improve in 24 to 48 hours need immediate surgery to remove all or most of the large intestine.
Maintenance regimens
To prevent symptoms from reappearing (that is, to maintain remission), people generally continue taking the medication that successfully treated their disease. However, if a steroid was used to treat their disease, the dose is lowered and they are eventually stopped (and a different medication used). Oral or rectal mesalamine is often used in combination with other medications as maintenance therapy.
Surgery
About 20 to 40% of people with extensive ulcerative colitis require surgery. Some reasons for surgery include chronic colitis that is disabling or that constantly requires high doses of steroids, cancer, and narrowing of the large intestine or growth failure in children. Emergency surgery may be necessary for sudden life-threatening attacks with massive bleeding, perforation, or fulminant colitis.
Complete removal of the large intestine, rectum, and anus (total proctocolectomy) permanently cures ulcerative colitis, restores life expectancy to normal, and eliminates the risk of colon cancer. However, inflammation develops in the small intestine in about 25% of people after surgery even though their small intestine was not previously affected.
The most common surgery is a procedure called proctocolectomy with ileal pouch-anal anastomosis (IPAA). In this procedure, the large intestine and most of the rectum are removed, and a small reservoir (pouch) is created out of the small intestine and attached to the remaining rectum just above the anus. Because the muscles of the anus (anal sphincter) are not removed, this procedure allows people to remain in control of their bowels (continence). However, because a small amount of tissue of the rectum can remain, the risk of cancer is significantly decreased but not eliminated.
A common complication of IPAA is inflammation of the reservoir (called pouchitis). To treat pouchitis, doctors give antibiotics. Most cases of pouchitis can be controlled with medications, but a small percentage cannot. For these cases, doctors create an ileostomy to correct the problem. In an ileostomy, a surgeon brings the end of the lowest portion of the small intestine (ileum) out through an opening in the abdominal wall (stoma). People who have an ileostomy must always wear a plastic bag (ileostomy bag) over the opening to collect the stool that comes out. An ileostomy used to be the traditional price of this cure.

Prognosis for Ulcerative Colitis
Ulcerative colitis is usually chronic, with repeated flare-ups and remissions (periods of no symptoms). In some people, an initial attack progresses rapidly and results in serious complications. In others, complete recovery occurs after a single attack. The remaining people have some degree of recurring disease.
People who have disease only in their rectum (ulcerative proctitis) have the best prognosis. Severe complications are unlikely. However, in some people, the disease eventually spreads to the large intestine (thus evolving into ulcerative colitis). In people who have ulcerative proctitis that has not spread, surgery is rarely required, cancer rates are not increased, and life expectancy is normal.
Colon cancer
The long-term survival rate for people with colon cancer caused by ulcerative colitis is about 75%. People are more likely to survive if the diagnosis is made during the early stages and the colon is removed in time.
More Information
The following English-language resources may be useful. Please note that The Manual is not responsible for the content of these resources.
Drug Information for the Topic





