

Ventricular fibrillation is a potentially fatal, uncoordinated series of very rapid, ineffective contractions of the ventricles (lower chambers of the heart) caused by many chaotic electrical impulses.
Ventricular fibrillation causes unconsciousness in seconds, and if the disorder is not rapidly treated, death follows.
Electrocardiography helps determine if the cause of cardiac arrest is ventricular fibrillation.
Cardiopulmonary resuscitation (CPR) must be started within a few minutes, and it must be followed by defibrillation (an electrical shock delivered to the chest) to restore normal heart rhythm.
(See also Overview of Abnormal Heart Rhythms.)
In ventricular fibrillation, the ventricles merely quiver and do not contract in a coordinated way. No blood is pumped from the heart, so ventricular fibrillation is a form of cardiac arrest. It causes death unless treated immediately.

The most common cause of ventricular fibrillation is a heart disorder, particularly inadequate blood flow to the heart muscle due to coronary artery disease, as occurs during a heart attack. Other causes include the following:
Shock (very low blood pressure), which can result from coronary artery disease and other disorders
Long QT syndrome (which may cause torsades de pointes ventricular tachycardia), including that due to very low levels of potassium in the blood (hypokalemia)
Medications that affect electrical currents in the heart (such as sodium channel blockers or potassium channel blockers—see table )
Idiopathic ventricular fibrillation
People who have been resuscitated from cardiac arrest caused by ventricular fibrillation typically are evaluated for heart disease, particularly coronary artery disease, cardiomyopathies, and channelopathies. If testing does not identify any causative disorder, the person is considered to have idiopathic ventricular fibrillation. Idiopathic means the cause is unknown.
Some of these people likely have an unrecognized or unknown genetic disorder. Because of the possibility that the disorder is genetic, doctors recommend that family members be examined for possible cardiac events (for example, fainting or palpitations) and that they undergo some testing, including electrocardiography, exercise stress testing, and echocardiography. It is unclear whether genetic testing is helpful.
People with idiopathic ventricular fibrillation are treated with an implantable cardioverter-defibrillator.
Symptoms of Ventricular Fibrillation
Ventricular fibrillation causes unconsciousness in seconds. If untreated, the person usually has a brief seizure and then becomes limp and unresponsive. People develop irreversible brain damage after about 5 minutes because oxygen no longer reaches the brain. Death soon follows.
Diagnosis of Ventricular Fibrillation
Electrocardiography

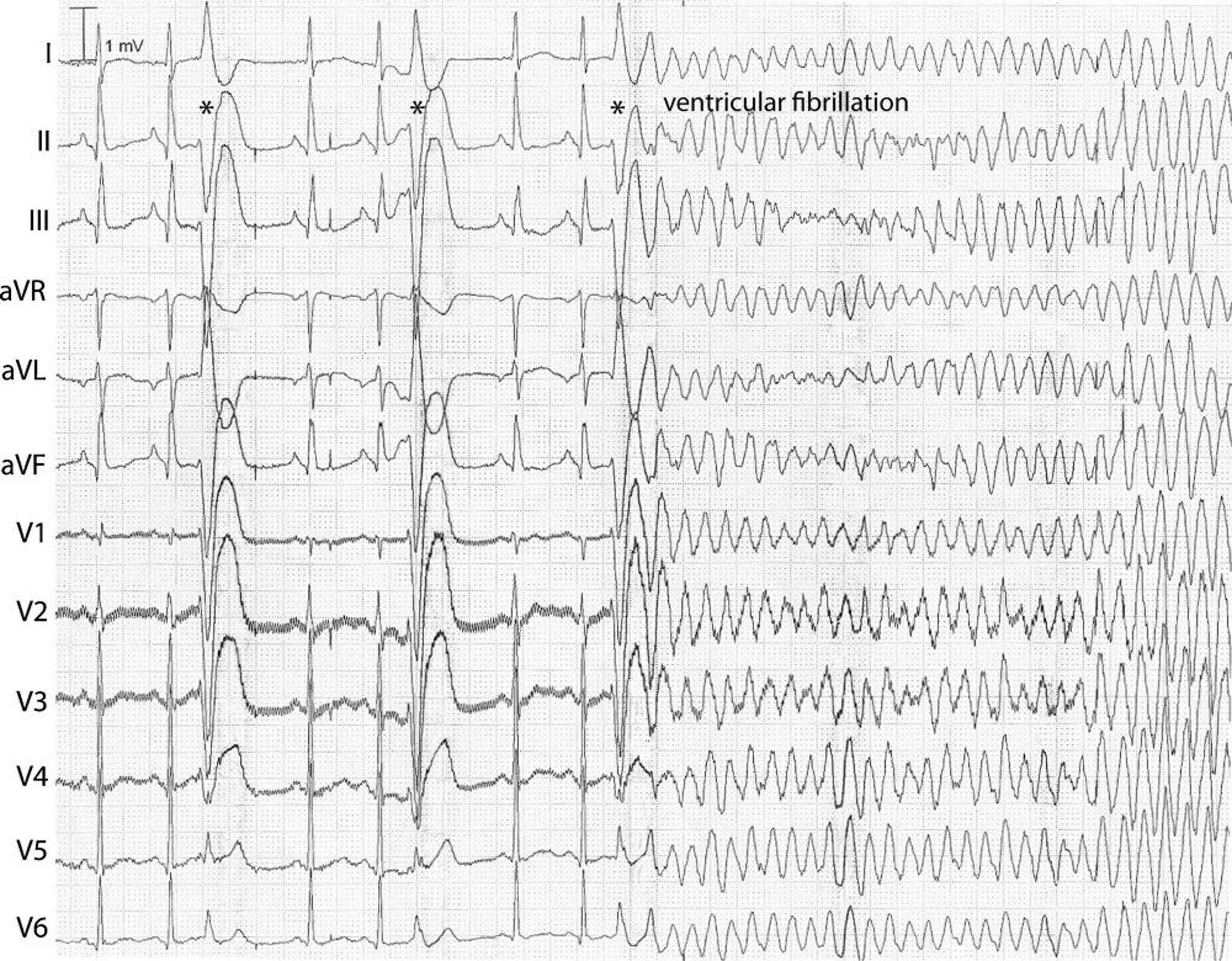
The right side of these strips show the ultrarapid and irregular, patternless beats that characterize ventricular fibrillation.
© Springer Science+Business Media
Cardiac arrest is diagnosed when a person suddenly collapses, turns deathly pale, stops breathing, and has no detectable pulse, heartbeat, or blood pressure. Ventricular fibrillation is diagnosed as the cause of the cardiac arrest by electrocardiography (ECG).
ECG: Reading the Waves
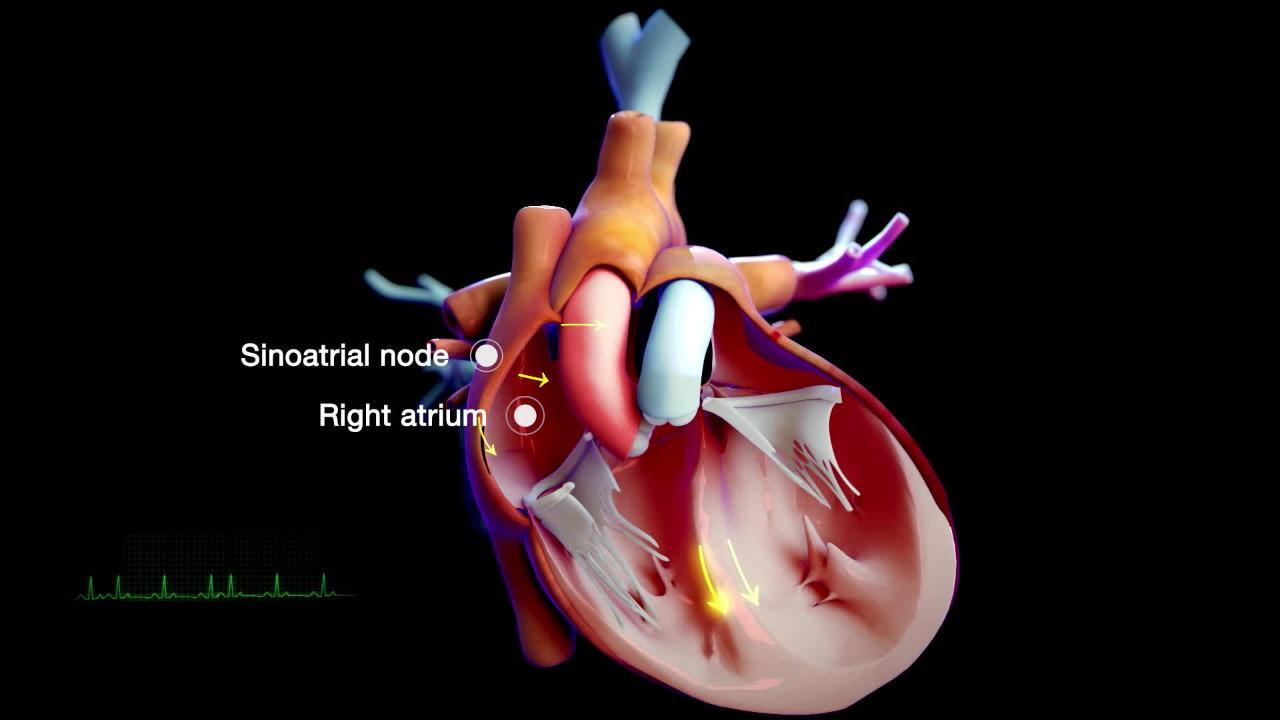
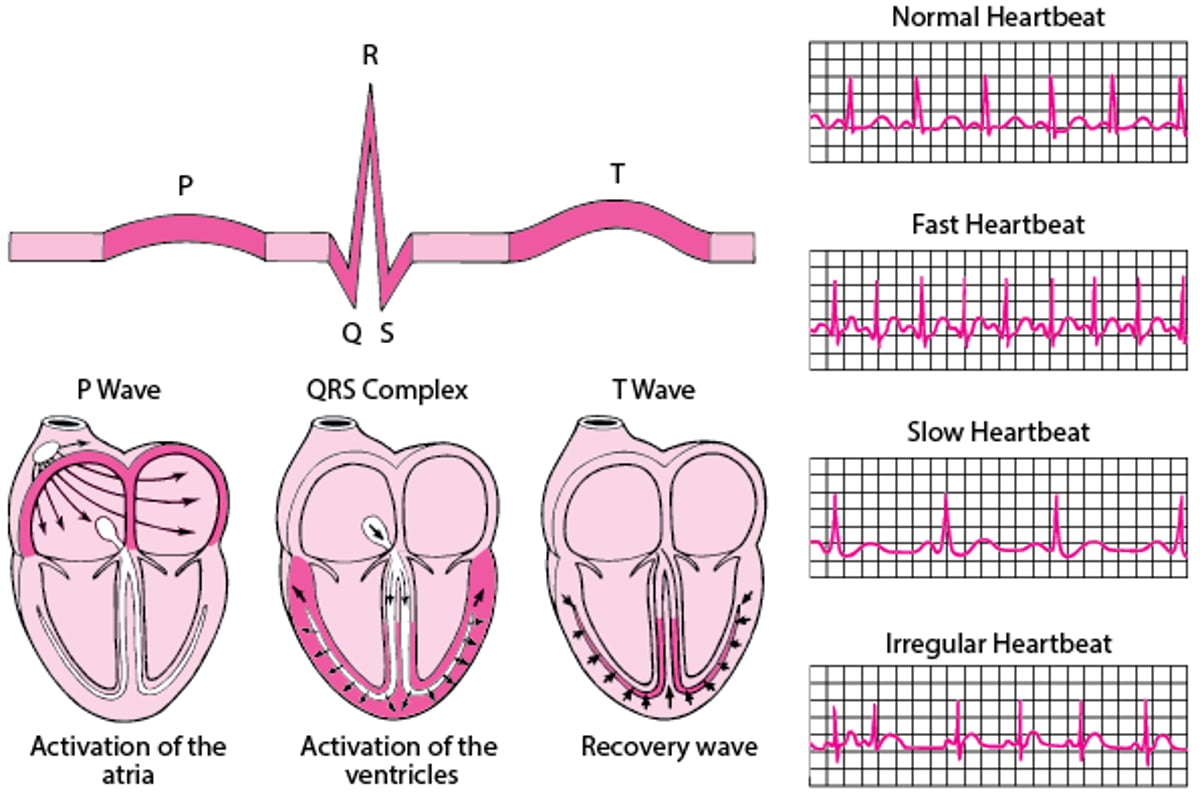
An electrocardiogram (ECG) represents the electrical current moving through the heart during a heartbeat. The current's movement is divided into parts, and each part is given an alphabetic designation in the ECG. Each heartbeat begins with an impulse from the heart's pacemaker (sinus or sinoatrial node). This impulse activates the upper chambers of the heart (atria). The P wave represents activation of the atria. Next, the electrical current flows down to the lower chambers of the heart (ventricles). The QRS complex represents activation of the ventricles. The electrical current then spreads back over the ventricles in the opposite direction. This activity is called the recovery wave, which is represented by the T wave. Many kinds of abnormalities can often be seen on an ECG. They include a previous heart attack (myocardial infarction), an abnormal heart rhythm (arrhythmia), an inadequate supply of blood and oxygen to the heart (ischemia), and excessive thickening (hypertrophy) of the heart's muscular walls. Certain abnormalities seen on an ECG can also suggest bulges (aneurysms) that develop in weak areas of the heart's walls. Aneurysms may result from a heart attack. If the rhythm is abnormal (too fast, too slow, or irregular), the ECG may also indicate where in the heart the abnormal rhythm starts. Such information helps doctors begin to determine the cause. |

Treatment of Ventricular Fibrillation
Cardiopulmonary resuscitation
Preventing further episodes
Ventricular fibrillation must be treated as an extreme emergency. Cardiopulmonary resuscitation (CPR) must be started as soon as possible. It must be followed by defibrillation (an electrical shock delivered to the chest), as soon as the defibrillator is available. Having automated external defibrillators (AEDs) available can thus be one of the most effective ways to save the lives of people who have cardiac arrest. Medications used to treat abnormal heart rhythms (see table ) may then be given to help maintain the normal heart rhythm.
When ventricular fibrillation occurs within a few hours of a heart attack in people who are not in shock and who do not have heart failure, prompt defibrillation restores normal rhythm in about 99% of people, and the prognosis is good. Shock and heart failure suggest severe damage to the ventricles. If the ventricles are severely damaged, even prompt cardioversion fails to resuscitate most people, and many people who are resuscitated die without regaining normal heart function.
People who are successfully resuscitated from ventricular fibrillation and survive are at high risk of another episode. If ventricular fibrillation is caused by a reversible disorder, that disorder is treated. Otherwise, most people have an implantable cardioverter-defibrillator (ICD) surgically implanted to give a shock to treat the fibrillation if it recurs. ICDs continually monitor the rate and rhythm of the heart, automatically detect ventricular fibrillation, and deliver a shock to convert the arrhythmia back to a normal rhythm. Such people are often also given medications to prevent recurrences.
More Information
The following English-language resource may be useful. Please note that The Manual is not responsible for the content of this resource.
American Heart Association: Arrhythmia: Information to help people understand their risks of arrhythmias as well as information on diagnosis and treatment





