





An estimated 1 to 3 per 100,000 apparently healthy young athletes develop an abrupt-onset heart rhythm abnormality and die suddenly during exercise. Males are affected up to 10 times more often than females. Basketball and football players in the United States and soccer players in Europe may be at highest risk.
Causes of Sudden Cardiac Death in Athletes
Generally, the causes of sudden death during exercise are very different in young athletes than in older athletes. However, in all athletes, asthma, heatstroke, and the use of performance-enhancing or recreational drugs may help trigger death due to sudden abnormal heart rhythms.
Young athletes
In young athletes, most sudden cardiac death occurs in people who have no abnormality of the heart structure. When there is an abnormality of heart structure, the most common one is abnormal thickening of the heart muscle (hypertrophic cardiomyopathy).
Other heart disorders that are present from birth, such as long QT syndrome or Brugada syndrome, cause abnormal heart rhythms and may also cause sudden death in young athletes.
Less commonly, undetected heart enlargement (dilated cardiomyopathy) may be present in a young person who has no symptoms, and the person may die suddenly during or after vigorous exercise. Inflammation of the heart muscle, usually due to a viral infection (myocarditis), can cause heart enlargement and abnormal rhythms, such as ventricular tachycardia, leading to sudden cardiac death.
Abnormalities of the coronary arteries, especially when one of the arteries takes an abnormal path through, rather than on top of, the heart muscle, may also cause sudden death in athletes when the compression cuts off blood flow to the heart during exercise.
Young athletes with inherited conditions, such as Marfan syndrome, that cause weakness in the wall of the aorta (the major artery leading from the heart) may develop a tear (aortic dissection) or a bulge (aortic aneurysm) that can rupture and lead to massive bleeding and sudden death.
Rarely, young, thin athletes may also have sudden heart rhythm disturbances if they experience a strong blow to the area directly over the heart (commotio cordis) even when they have no heart disorder. The blow often involves a fast-moving projectile such as a baseball, hockey puck, or lacrosse ball or impact with another player.
Older athletes
In older athletes, the most common cause is
Occasionally, hypertrophic cardiomyopathy or heart valve disease is a cause. The causes common in younger athletes may also be causes in older athletes.
Symptoms of Sudden Cardiac Death in Athletes
Some athletes have warning signs such as fainting or shortness of breath. Often, however, athletes do not recognize or report these symptoms, and the first sign is that the person suddenly stops breathing and collapses.
Treatment of Sudden Cardiac Death in Athletes
Resuscitation
If people stop breathing and collapse, immediate treatment is with
Use of an automated external defibrillator if available
Resuscitation is continued in the emergency department. If the person survives, doctors treat the condition that caused the abnormal rhythm. Sometimes doctors place an implantable cardioverter-defibrillator, which continually monitors the person's heart rhythm and delivers a shock to return the rhythm to normal if needed.
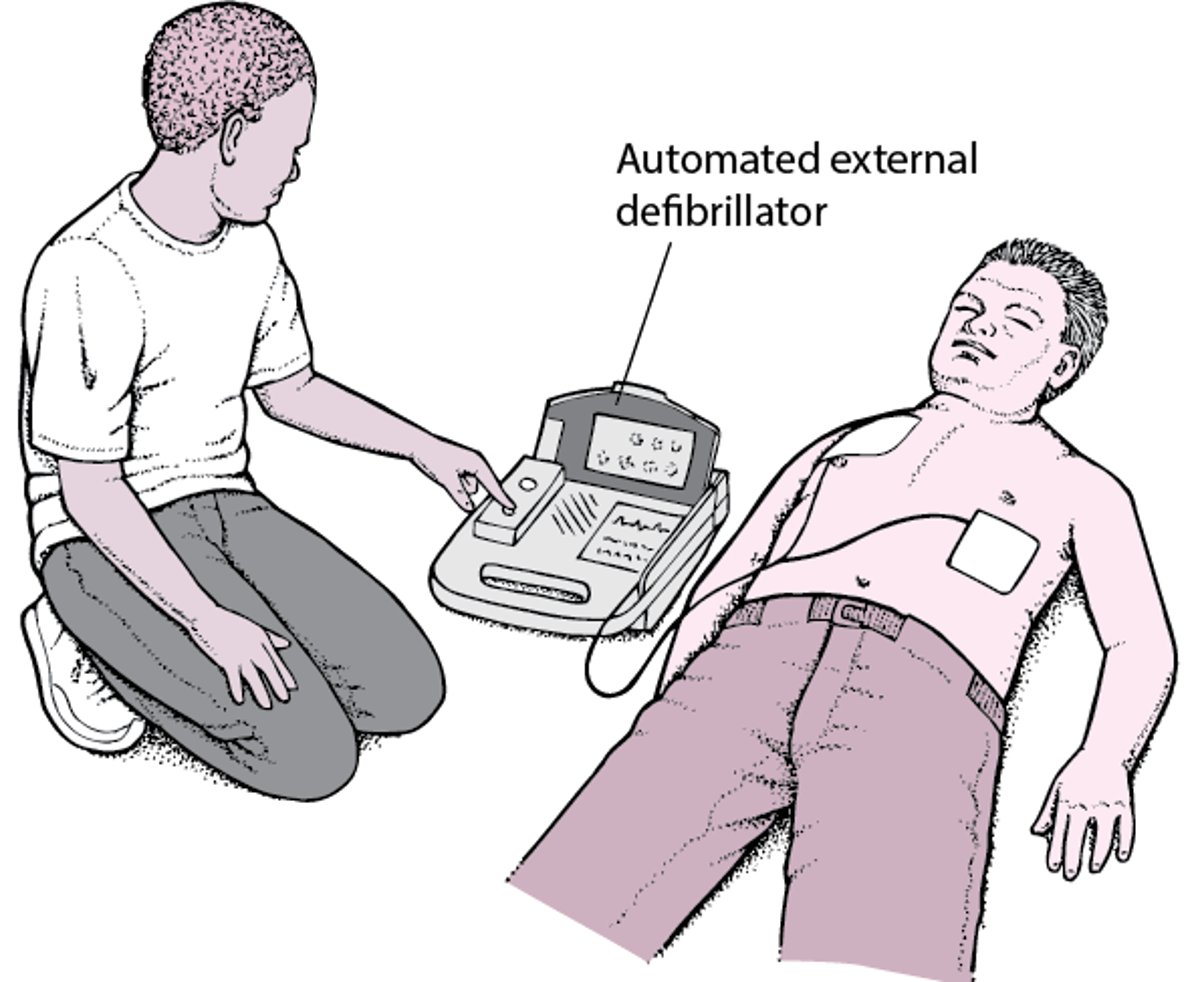
Automated External Defibrillator: Jump-Starting the Heart
An automated external defibrillator (AED) is a device that can detect and correct a type of abnormal heart rhythm called ventricular fibrillation. Ventricular fibrillation causes cardiac arrest. AEDs are easy to use. Many organizations provide training sessions on the use of AEDs. Most training sessions take only a few hours, but it is possible to use an AED even if you have never participated in a training course. Different AEDs have somewhat different instructions for use. The instructions are written on the AED, and most AEDs also use voice prompts to direct the user in each step. AEDs are available in many public gathering places, such as stadiums, airports, and concert halls. People who are told by their doctor that they are likely to develop ventricular fibrillation but who do not have an implanted defibrillator may want to purchase an AED for home use by family members, who should be trained in its use. |

More Information
The following English-language resource may be useful. Please note that THE MANUAL is not responsible for the content of this resource.
Nick of Time Foundation: This organization works to increase survival of sudden cardiac arrest with awareness, "hands-only" CPR training, advocacy for having defibrillators in all public places, and access to screening for young athletes.





