

Strokes are a heterogeneous group of disorders involving sudden, focal interruption of cerebral blood flow that causes neurologic deficit. Strokes can be
Ischemic (80%), typically resulting from thrombosis or embolism
Hemorrhagic (20%), resulting from vascular rupture (eg, subarachnoid hemorrhage, intracerebral hemorrhage)
Sudden transient neurologic dysfunction caused by focal brain, spinal cord, or retinal ischemia (typically lasting < 1 hour), without evidence of acute cerebral infarction (based on diffusion-weighted MRI) is termed a transient ischemic attack (TIA) (1, 2).
In the United States, stroke is the fifth most common cause of death and the most common cause of neurologic disability in adults.

Strokes involve the arteries of the brain (see figure ), either the anterior circulation (branches of the internal carotid artery) or the posterior circulation (branches of the vertebral and basilar arteries).
Arteries of the Brain
The anterior cerebral artery supplies the medial portions of the frontal and parietal lobes and corpus callosum. The middle cerebral artery supplies large portions of the lateral surfaces of frontal, parietal, and temporal lobes. Branches of the anterior and middle cerebral arteries (lenticulostriate arteries) supply the basal ganglia and anterior limb of the internal capsule. The vertebral and basilar arteries supply the brain stem, cerebellum, posterior cerebral cortex, and medial temporal lobe. The posterior cerebral arteries bifurcate from the basilar artery to supply the medial temporal (including the hippocampus) and occipital lobes, thalamus, and mammillary and geniculate bodies. Anterior circulation and posterior circulation communicate in the circle of Willis via the posterior communicating artery. |


Risk factors
The following are modifiable risk factors that contribute to increased risk of stroke:
Cigarette smoking
Insulin resistance
Abdominal obesity
Lack of physical activity
High-risk diet (eg, high in saturated fats, trans fats, and calories)
Psychosocial stress (eg, depression)
Heart disorders (particularly disorders that predispose to emboli, such as acute myocardial infarction, valvular heart disease, infective endocarditis, and atrial fibrillation)
Carotid artery stenosis
Hypercoagulability (thrombotic stroke only)
Intracranial aneurysms (subarachnoid hemorrhage only)
Use of certain drugs (eg, cocaine, amphetamines)Use of certain drugs (eg, cocaine, amphetamines)
Anticoagulants and antiplatelet medications
Use of estrogen therapy, including oral contraceptives
Unmodifiable risk factors include the following:
Prior stroke
Older age
Family history of stroke
Race and ethnicity
Genetic factors
References
1. Kokotailo RA, Hill MD. Coding of stroke and stroke risk factors using international classification of diseases, revisions 9 and 10. Stroke. 2005 Aug;36(8):1776-81. doi: 10.1161/01.STR.0000174293.17959.a1. Epub 2005 Jul 14
2. Sacco RL, Kasner SE, Broderick JP, et al. An updated definition of stroke for the 21st century: a statement for healthcare professionals from the American Heart Association/American Stroke Association [published correction appears in Stroke. 2019 Aug;50(8):e239. doi: 10.1161/STR.0000000000000205.]. Stroke. 2013;44(7):2064-2089. doi:10.1161/STR.0b013e318296aeca
Symptoms and Signs of Stroke
Initial symptoms of stroke occur suddenly. Symptoms depend on the location of infarction (see figure Areas of the Brain by Function).
Thus, symptoms can include numbness, weakness of limbs or face; aphasia; confusion; visual disturbances in one or both eyes (eg, transient monocular blindness, diplopia); dizziness or loss of balance and coordination; and headache.
Areas of the Brain by Function

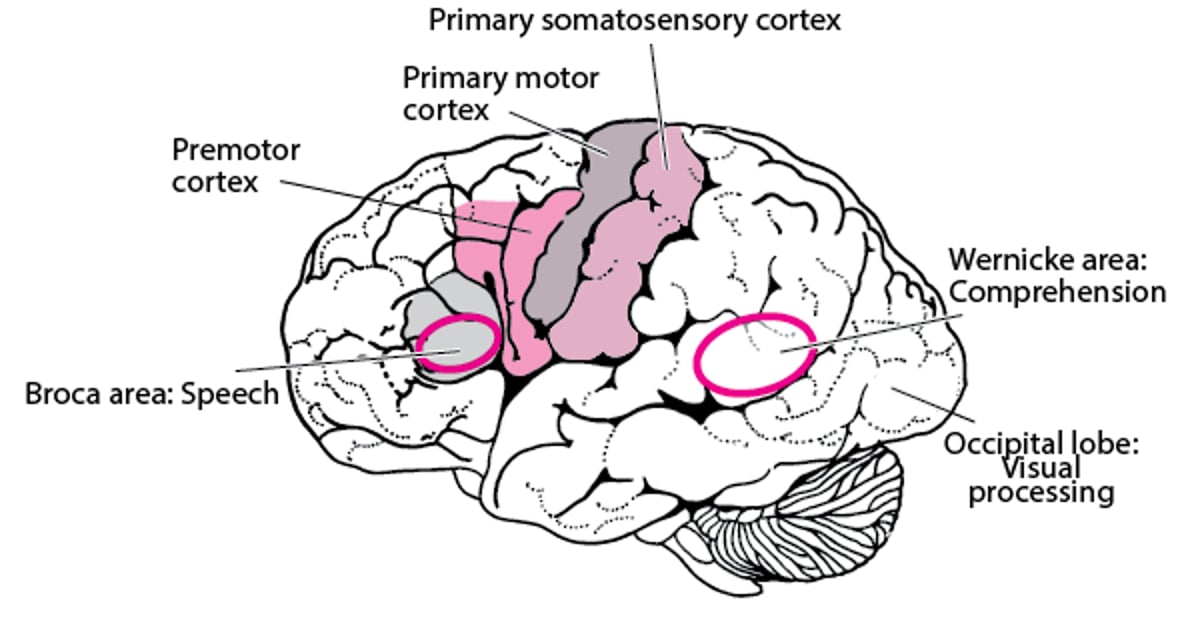
Neurologic deficits are used to determine the location of stroke (see table ). Anterior circulation stroke typically causes unilateral symptoms. Posterior circulation stroke can cause unilateral or bilateral deficits and is more likely to affect consciousness, especially when the basilar artery is involved.
Selected Stroke Syndromes
Symptoms and Signs | Syndrome |
|---|---|
Contralateral hemiparesis (maximal in the leg), urinary incontinence, apathy, confusion, poor judgment, mutism, grasp reflex, gait apraxia | Anterior cerebral artery |
Contralateral hemiparesis (worse in the arm and face than in the leg), dysarthria, hemianesthesia, contralateral homonymous hemianopia, aphasia (if the dominant hemisphere is affected) or apraxia and sensory neglect (if the nondominant hemisphere is affected) | Middle cerebral artery |
Contralateral homonymous hemianopia, unilateral cortical blindness, memory loss, unilateral 3rd cranial nerve palsy, hemiballismus | Posterior cerebral artery |
Monocular loss of vision (amaurosis) | Ophthalmic artery (a branch of the internal carotid artery) |
Unilateral or bilateral cranial nerve deficits (eg, nystagmus, vertigo, dysphagia, dysarthria, diplopia, blindness), truncal or limb ataxia, spastic paresis, crossed sensory and motor deficits*, impaired consciousness, coma, death (if basilar artery occlusion is complete), tachycardia, labile blood pressure | Vertebrobasilar system |
Absence of cortical deficits plus one of the following:
| Lacunar infarcts |
* Ipsilateral facial sensory loss or motor weakness with contralateral body hemianesthesia or hemiparesis indicates a lesion at the pons or medulla. | |
Systemic or autonomic disturbances (eg, hypertension, fever) occasionally occur.
Other manifestations, rather than neurologic deficits, often suggest the type of stroke. For example:
Sudden, severe headache suggests subarachnoid hemorrhage.
Impaired consciousness or coma, often accompanied by headache, nausea, and vomiting, suggests increased intracranial pressure, which can occur 48 to 72 hours after large ischemic strokes and earlier in many hemorrhagic strokes; fatal brain herniation may result.
Complications
Stroke complications can include sleep problems, confusion, depression, incontinence, atelectasis, pneumonia, and swallowing dysfunction, which can lead to aspiration, dehydration, or undernutrition. Immobility can lead to thromboembolic disease, deconditioning, sarcopenia, urinary tract infections, pressure ulcers, and contractures.
Daily functioning (including the ability to walk, see, feel, remember, think, and speak) may be decreased.
Evaluation of Stroke
Evaluation aims to establish the following:
Whether stroke has occurred
Whether stroke is ischemic or hemorrhagic
Whether emergency treatment is required
What the best strategies for preventing subsequent strokes are
Whether and how to pursue rehabilitation
Stroke is suspected in patients with any of the following:
Sudden neurologic deficits compatible with brain damage in an arterial territory
A particularly sudden, severe headache
Sudden, unexplained coma
Sudden impairment of consciousness
When stroke is suspected, clinicians may use standardized criteria to grade severity and follow changes over time. This approach can be particularly useful as an outcome measure in efficacy studies. The National Institutes of Health Stroke Scale (NIHSS) is often used. It is a 15-item scale to evaluate the patient's level of consciousness and language function and to identify motor and sensory deficits by asking the patient to answer questions and to perform physical and mental tasks. It is also useful for choosing appropriate treatment and predicting outcome.
Testing
Glucose is measured at bedside to rule out hypoglycemia. Measurement of blood glucose is the only blood test needed for all patients before thrombolytics are given. However, if the patient is receiving an anticoagulant, platelet count, international normalized ratio (INR), and partial thromboplastin time are measured.
If stroke is still suspected, immediate neuroimaging is required to differentiate hemorrhagic from ischemic stroke and to detect signs of increased intracranial pressure.
CT without angiogram is sensitive for intracranial blood but may be normal or show only subtle changes during the first hours of symptoms after anterior circulation ischemic stroke. CT also misses some small posterior circulation strokes. MRI is sensitive for intracranial blood and may detect signs of ischemic stroke missed by CT, but CT can usually be performed more rapidly. If CT does not confirm clinically suspected stroke, diffusion-weighted MRI can usually detect ischemic stroke.
Imaging of the cervical and intracranial vessels is generally recommended as a part of the routine workup to determine etiology and guide further management. Guidelines recommend that all patients with clinical suspicion of large vessel occlusion should undergo vessel imaging (CTA or MRA), especially within 24 hours of symptom onset given advances in acute stroke treatment.

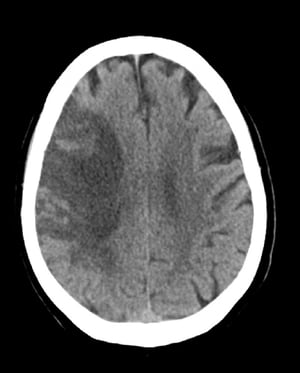
This image shows low attenuation in the distribution of the right middle cerebral artery consistent with a subacute ischemic stroke with hemorrhage developing in areas of ischemia.
This image shows low attenuation in the distribution of the right middle cerebral artery consistent with a subacute isc
© 2017 Elliot K. Fishman, MD.

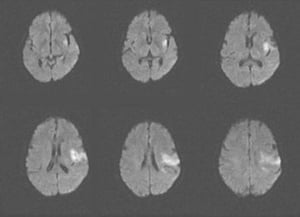
This MRI scan shows an area of restricted diffusion consistent with an acute ischemic stroke in the left insular and frontal lobes.
This MRI scan shows an area of restricted diffusion consistent with an acute ischemic stroke in the left insular and fr
Image courtesy of Ji Y. Chong, MD.

This noncontrast head CT scan shows a hyperdense left middle cerebral artery. This finding indicates a focal clot in the left middle cerebral artery (arrow).
This noncontrast head CT scan shows a hyperdense left middle cerebral artery. This finding indicates a focal clot in th
Image courtesy of Ji Y. Chong, MD.
This image shows low attenuation in the distribution of the right middle cerebral artery consistent with a subacute ischemic stroke with hemorrhage developing in areas of ischemia.
This image shows low attenuation in the distribution of the right middle cerebral artery consistent with a subacute isc
© 2017 Elliot K. Fishman, MD.
This MRI scan shows an area of restricted diffusion consistent with an acute ischemic stroke in the left insular and frontal lobes.
This MRI scan shows an area of restricted diffusion consistent with an acute ischemic stroke in the left insular and fr
Image courtesy of Ji Y. Chong, MD.
This noncontrast head CT scan shows a hyperdense left middle cerebral artery. This finding indicates a focal clot in the left middle cerebral artery (arrow).
This noncontrast head CT scan shows a hyperdense left middle cerebral artery. This finding indicates a focal clot in th
Image courtesy of Ji Y. Chong, MD.
If consciousness is impaired and lateralizing signs are absent or equivocal, further testing is performed to check for causes other than stroke (eg, postictal state, metabolic encephalopathies, drugs and toxins):
Blood tests: Comprehensive metabolic panel (including at least serum electrolytes, blood urea nitrogen [BUN], creatinine, blood glucose, and calcium levels), complete blood count (CBC) with differential and platelets, liver tests, and ammonia level
Arterial blood gases (ABGs)
Blood and urine culture and routine toxicology
Electrocardiography (ECG) to check for myocardial infarction and new arrhythmias
Chest radiograph to check for new lung disease that may affect brain oxygenation.
Imaging tests to check for masses, hemorrhage, edema, evidence of bone trauma, and hydrocephalus (first, noncontrast head CT, followed by MRI or contrast CT if needed for diagnosis)
Echocardiography to check the heart for blood clots, pumping or structural abnormalities, and valve disorders
Electroencephalography
After the stroke is identified as ischemic or hemorrhagic, tests are performed to determine the cause. Patients are also evaluated for coexisting acute general disorders (eg, infection, dehydration, hypoxia, hyperglycemia, hypertension). Patients are asked about depression, which commonly occurs after stroke. A dysphagia team evaluates swallowing; sometimes a barium swallow study is necessary.

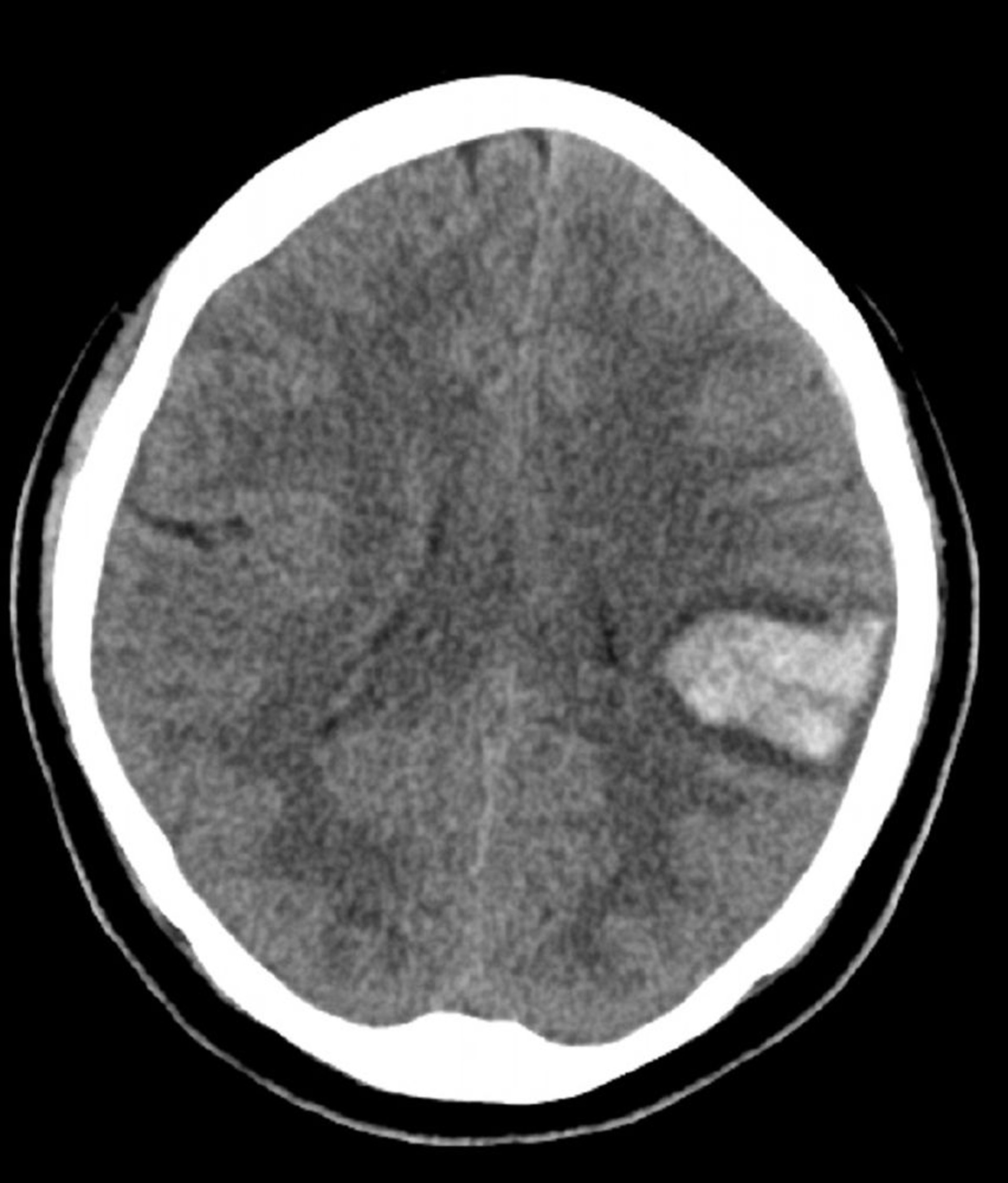
Increased density in the left brain seen on this noncontrast CT is consistent with intracerebral hemorrhage.
© 2017 Elliot K. Fishman, MD.
Treatment of Stroke
Treatment of stroke focuses on interventions to address different needs in the immediate, acute, and convalescent phases of illness, as follows (1):
Stabilization
Reperfusion for some ischemic strokes
Supportive measures and treatment of complications
Strategies to prevent future strokes
Rehabilitation
Stabilization may need to precede complete evaluation. Comatose or obtunded patients (eg, Glasgow Coma Score ≤ 8) may require airway support. If increased intracranial pressure is suspected, intracranial pressure monitoring and measures to reduce cerebral edema may be necessary.
Specific acute treatments vary by type of stroke. They may include reperfusion (eg, IV thrombolysis, mechanical thrombectomy) for some ischemic strokes.

Providing supportive care, correcting coexisting abnormalities (eg, fever, hypoxia, dehydration, hyperglycemia, sometimes hypertension), and preventing and treating complications are vital during the acute phase and convalescence (see table ); these measures clearly improve clinical outcomes (2). During convalescence, measures to prevent aspiration, deep venous thrombosis, urinary tract infections, pressure ulcers, and undernutrition may be necessary. Passive exercises, particularly of paralyzed limbs, and breathing exercises are started early to prevent contractures, atelectasis, and pneumonia.
Strategies to Prevent and Treat Stroke Complications
Applying intermittent external leg compression devices when anticoagulants are contraindicated and providing frequent active and passive leg exercises |
Turning bedridden patients frequently, with special attention to pressure sites |
Passively moving limbs at risk of contractures and placing them in the appropriate resting positions, using splints if necessary |
Ensuring adequate fluid intake and nutrition, including evaluating patients for swallowing difficulties and providing nutritional support as necessary |
Giving small doses of enoxaparin 40 mg subcutaneously every 24 hours or heparin 5000 U subcutaneously every 12 hours, when not contraindicated, to prevent deep venous thrombosis and pulmonary embolismGiving small doses of enoxaparin 40 mg subcutaneously every 24 hours or heparin 5000 U subcutaneously every 12 hours, when not contraindicated, to prevent deep venous thrombosis and pulmonary embolism |
Encouraging early ambulation (as soon as vital signs are normal), with close monitoring |
Maximizing lung function (eg, smoking cessation, deep breathing exercises, respiratory therapy, measures to prevent aspiration in patients with dysphagia) |
Looking for and treating infections early, especially pneumonia, urinary tract infections, and skin infections |
Managing urinary bladder problems in bedbound patients, preferably without using an indwelling catheter |
Promoting risk factor modification (eg, smoking cessation, weight loss, healthful diet) |
Prescribing early rehabilitation (eg, active and passive exercises, range-of-motion exercises) |
Compassionately discussing residual function, prognosis for recovery, and strategies to compensate for lost function with the patient and family/caregivers |
Encouraging maximum independence through rehabilitation |
Encouraging the patient and family members to contact stroke support groups for social and psychologic support |
After a stroke, most patients require rehabilitation (occupational and physical therapy) to maximize functional recovery. Some need additional therapies (eg, speech therapy, feeding restrictions). For rehabilitation, an interdisciplinary approach is best.
Depression after stroke may require antidepressants; many patients benefit from counseling.
Modifying risk factors through lifestyle changes (eg, stopping cigarette smoking) and medications (eg, for hypertension) can help delay or prevent subsequent strokes. Other stroke prevention strategies are chosen based on the patient's risk factors. For ischemic stroke prevention, strategies may include procedures (eg, carotid endarterectomy, stent placement), antiplatelet therapy, and anticoagulation.
Treatment references
1. Mead GE, Sposato LA, Sampaio Silva G, et al. A systematic review and synthesis of global stroke guidelines on behalf of the World Stroke Organization. Int J Stroke. 2023;18(5):499-531. doi:10.1177/17474930231156753
2. Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals From the American Heart Association/American Stroke Association [published correction appears in Stroke. 2019 Dec;50(12):e440-e441. doi: 10.1161/STR.0000000000000215.]. Stroke. 2019;50(12):e344-e418. doi:10.1161/STR.0000000000000211
Prognosis for Stroke
The sooner a stroke is treated, the less severe brain damage is likely to be and the better the chances for recovery.
Certain factors, such as type of stroke, older age, and pre-stroke functional dependence, suggest a poor outcome. Strokes that impair consciousness or that affect a large part of the left side of the brain may be particularly grave (1).
Usually, the more quickly patients improve during the days after stroke, the more they will ultimately improve. Improvement commonly continues for 6 to 12 months after the stroke. In adults who have had an ischemic stroke, problems that remain after 12 months are likely to be permanent, but children continue to improve slowly for many months. Older adults fare less well than younger people. For people who already have other serious disorders (eg, dementia), recovery is more limited.
Among all types of strokes, lacunar strokes have the best prognosis.
Compared with ischemic stroke, hemorrhagic stroke is associated with a poorer functional outcome, greater functional dependence, and lower survival. Nevertheless, if a hemorrhagic stroke is not massive and intracranial hypertension is absent, the outcome is likely to be better than that after an ischemic stroke with similar symptoms. Blood (in a hemorrhagic stroke) does not damage brain tissue as much as ischemia does.
Prognosis reference
1. Sennfält S, Norrving B, Petersson J, et al. Long-Term Survival and Function After Stroke: A Longitudinal Observational Study From the Swedish Stroke Register. Stroke. 2019;50(1):53-61. doi:10.1161/STROKEAHA.118.022913
Drug Information for the Topic





