



In seizure disorders, the brain's electrical activity is periodically disturbed, resulting in some degree of temporary brain dysfunction.
Many people have unusual sensations just before a seizure starts.
Some seizures cause uncontrollable shaking and loss of consciousness, but sometimes people simply stop moving or become unaware of what is happening.
Doctors suspect the diagnosis based on symptoms, but imaging of the brain, blood tests, and electroencephalography (to record the brain’s electrical activity) are usually needed to identify the cause.
If needed, medications can usually help prevent seizures.
Normal brain function requires an orderly, organized, coordinated discharge of electrical impulses. Electrical impulses enable the brain to communicate with the spinal cord, nerves, and muscles as well as within itself. Seizures may result when the brain’s electrical activity is disrupted.
About 8 to 10% of people will have a seizure at some time during their life; 2 to 4% of them will have epilepsy. Seizure disorders commonly begin in early childhood or in late adulthood.
Types of seizures
Seizures may be described as follows:
Epileptic: These seizures have no apparent trigger (that is, they are unprovoked), and they occur 2 or more times. One seizure is not considered epilepsy. Epileptic seizures are called a seizure disorder or epilepsy. The cause of epileptic seizures is often unknown (called idiopathic epilepsy). But sometimes they may be caused by various brain disorders, such as structural abnormalities, strokes, or tumors. In such cases, they are called symptomatic epilepsy. Symptomatic epilepsy is most common among newborns and older people.
Nonepileptic: These seizures are triggered (provoked) by a reversible disorder or a temporary condition that irritates the brain, such as an infection, a head injury, or a reaction to a medication. In children, a fever can trigger a nonepileptic seizure (called a febrile seizure).
Certain mental disorders can cause symptoms that resemble seizures, called psychogenic nonepileptic seizures or functional seizures (previously referred to as pseudoseizures).
Causes of Seizure Disorders
Which causes are most common depend on when seizures start:
Before age 2: High fevers or temporary metabolic abnormalities, such as an abnormal blood level of sugar (glucose), calcium, magnesium, vitamin B6, or sodium, can trigger 1 or more seizures. Seizures do not recur once the fever or abnormality resolves. If the seizures recur without such triggers, the cause is likely to be an injury during birth, a birth defect, a hereditary metabolic abnormality, a or brain disorder.
2 to 14 years: Often, the cause is unknown (see also Seizures in Children).
Adults: A head injury, stroke, or tumor may damage the brain, causing a seizure. Alcohol withdrawal (caused by suddenly stopping drinking) is a common cause of seizures. However, in about half of adults with seizures, the cause is unknown.
Older adults: The cause may be a brain tumor or stroke.
Seizures with no identifiable cause are called idiopathic.
Conditions that irritate the brain—such as injuries, certain medications, sleep deprivation, infections, fever—or that deprive the brain of oxygen or fuel—such as abnormal heart rhythms, a low level of oxygen in the blood, or a very low level of sugar in the blood (hypoglycemia)—can trigger a single seizure whether a person has a seizure disorder or not. A seizure that results from such a stimulus is called a provoked seizure (and thus is a nonepileptic seizure).
People with a seizure disorder are more likely to have a seizure when:
They are under excess physical or emotional stress.
They are intoxicated or deprived of sleep.
They habitually drink alcohol or regularly take sedatives and suddenly stop drinking or using sedatives.
Avoiding these conditions can help prevent seizures.
Rarely, seizures are triggered by repetitive sounds, flashing lights, video games, or even touching certain parts of the body. In such cases, the disorder is called reflex epilepsy.
Causes of Seizures
Cause | Examples |
|---|---|
High fever | Infections |
Viral encephalitis | |
Metabolic disorders | High blood levels of sugar (hyperglycemia) or sodium Low blood levels of sugar (hypoglycemia), calcium, magnesium, or sodium |
Other disorders | Kidney failure or liver failure, which can lead to dysfunction of the brain (encephalopathy) Vitamin B6 deficiency (in newborns) |
Inadequate oxygen supply to the brain | Near suffocation |
Structural damage to the brain | Brain tumor (noncancerous or cancerous) Intracranial hemorrhage (bleeding within the skull) Stroke |
Abnormalities present or occurring at birth, including genetic disorders | Hereditary metabolic disorders, such as Tay-Sachs disease or phenylketonuria |
Fluid accumulation in the brain (cerebral edema) | Cerebral venous thrombosis |
Medications* | Buspirone (used to treat anxiety disorders)Buspirone (used to treat anxiety disorders) CamphorCamphor *Cefepime (an antibiotic)*Cefepime (an antibiotic) *Chlorpromazine (used to treat schizophrenia)*Chlorpromazine (used to treat schizophrenia) Ciprofloxacin (an antibiotic)Ciprofloxacin (an antibiotic) Chloroquine (used to treat malaria)Chloroquine (used to treat malaria) Clozapine (used to treat schizophrenia)Clozapine (used to treat schizophrenia) Cyclosporine (used to prevent and treat rejection of organ transplants)Cyclosporine (used to prevent and treat rejection of organ transplants) Imipenem (an antibiotic) *Indomethacin (used to relieve pain and reduce inflammation)*Indomethacin (used to relieve pain and reduce inflammation) *Meperidine (used to relieve pain)*Meperidine (used to relieve pain) *Phenytoin†*Phenytoin† Theophylline (used to treat asthma and other airway disorders)Theophylline (used to treat asthma and other airway disorders) TramadolTramadol Tricyclic antidepressants |
Illicit drugs | Cocaine (overdose) |
Withdrawal of a medication or substance after heavy use | General anesthetics (used during surgery) Sedatives, including sleep aids |
Exposure to toxins | Strychnine |
* Various medications can cause seizures if too much is taken. In some people, certain medications can make seizures more likely to occur by making nerve cells in the brain easier to stimulate. These medications are thought to lower the seizure threshold. | |
† Phenytoin, used to treat seizure disorders, can cause seizures if too much is taken.† Phenytoin, used to treat seizure disorders, can cause seizures if too much is taken. | |
Symptoms of Seizure Disorders
An aura (unusual sensations) describes how a person feels before a seizure starts. An aura may include any of the following:
Abnormal smells or tastes
Butterflies in the stomach
Feeling as if something has been experienced before even though it has not (called déjà vu) or the opposite feeling—something seems unfamiliar even though it is familiar in some way (called jamais vu)
An intense feeling that a seizure is about to begin
Almost all seizures are relatively brief, lasting from a few seconds to a few minutes. Most seizures last 1 to 2 minutes.
Occasionally, seizures recur repeatedly, as occurs in status epilepticus.
Most people who have a seizure disorder look and behave normally between seizures.
Symptoms of seizures vary depending on which area of the brain is affected by the abnormal electrical discharge, as in the following:
An intensely pleasant or unpleasant taste if the part of the cerebrum called the insula is affected
Visual hallucinations (seeing unformed images) if the occipital lobe is affected
Inability to speak if the area that controls speech (located in the frontal lobe) is affected
A convulsion (jerking and spasms of muscles throughout the body) if large areas on both sides of the brain are affected
Seizures may be classified as
Motor: Involving abnormal muscle contractions (such as jerking of a limb or convulsions)
Nonmotor: Not involving abnormal muscle contractions
Other possible symptoms include numbness or tingling in a specific body part, brief episodes of unresponsiveness, loss of consciousness, and confusion. People may vomit if they lose consciousness. People may lose control of their muscles, bladder, or bowels. Some people bite their tongue.
Symptoms also vary depending on whether the seizure is
Focal-onset (the seizure begins in 1 side of the brain)
Generalized-onset (the seizure begins in both sides of the brain)
There are several types of focal and generalized seizures. Most people have only 1 type of seizure. Others have 2 or more types.
Some types of seizures may be focal, then become generalized.


The first panel of this illustration shows a healthy brain with a normal wave pattern and no seizure activity.
The second panel shows the wave pattern of a person with a focal-seizure disorder and where in the brain it occurs. A focal seizure begins in 1 side of the brain.
The third panel shows the wave pattern of a generalized seizure and where in the brain it occurs. A generalized seizure begins in both sides of the brain.
Note: Seizures, by definition, last at least 10 seconds; abnormal EEG patterns shown here would be more prolonged.
vishalgokulwale/stock.adobe.com
Focal-onset seizures
In focal-onset seizures, the seizures begin in 1 side of the brain.
Focal-onset seizures include the following types:
Automatisms (coordinated, purposeless, repetitive motor activity)
Atonic (involving loss of muscle tone)
Clonic (involving rhythmic jerking of muscles)
Epileptic spasms (involving bending and straightening the arms and bending the upper body forward) in children
Hyperkinetic (involving moving the legs as if pedaling a bicycle or thrashing)
Myoclonic (involving sudden, lightning-like jerking of muscles)
Tonic (involving stiffening of muscles of 1 limb or 1 side of the body)
Some people have a focal-onset seizure that resolves. In others, the abnormal electrical discharge spreads to adjacent areas and to the other side of the brain, resulting in a generalized seizure. Generalized seizures that result from focal seizures are called focal-to-bilateral seizures. That is, they start in 1 side of the brain and spread to both sides.
Focal-onset seizures are classified based on whether or not the person is fully conscious (aware of what is going on in the body and environment) during the seizure:
Focal preserved-consciousness seizures (formerly called focal-aware seizures).
Focal impaired-consciousness seizures (formerly called focal impaired-awareness seizures).
Consciousness refers to knowledge of self and environment and the ability to respond to both. If consciousness is impaired during any part of the seizure, the seizure is considered a focal impaired-consciousness seizure. Doctors determine whether people remained conscious during a seizure by asking them or, if a seizure is occurring, seeing whether they respond when spoken to.
In focal preserved-consciousness seizures, abnormal electrical discharges begin in a small area of the brain and remain confined to that area. Because only a small area of the brain is affected, symptoms are related to the function controlled by that area. For example, if the small area of the brain that controls the right arm’s movements (in the left frontal lobe) is affected, the right arm may involuntarily lift up and jerk, and the head may turn toward the lifted arm. People are completely conscious and aware of the surroundings. A focal preserved-consciousness seizure may progress to a focal impaired-consciousness seizure.
Jacksonian seizures are a type of focal preserved-consciousness seizures. Symptoms start in 1 hand or foot, then move up the limb as the electrical activity spreads in the brain. People are completely aware of what is occurring during the seizure.
Other focal preserved-consciousness seizures affect the face, then spread to an arm or sometimes a leg.
Epilepsia partialis continua is rare. In this type of preserved-consciousness seizure, focal seizures occur every few seconds or minutes for days to years at a time. They typically affect an arm, a hand, 1 side of the face, or 1 side of the body. People with epilepsia partialis continua remain conscious. Examples of causes of these seizures include:
In adults: Brain damage (such as scarring due to a stroke or tumor) in 1 area of the brain
In children: Inflammation of the brain (as occurs in encephalitis and measles)
In focal impaired-consciousness seizures, abnormal electrical discharges usually begin in a small area of the temporal lobe or frontal lobe and quickly spread to other nearby areas. The seizures usually begin with an aura, which lasts 1 to 2 minutes. During the aura, people start to lose touch with the surroundings.
During focal impaired-consciousness seizures, awareness becomes impaired, but people do not become unconscious. People may do the following:
Stare
Chew or smack the lips involuntarily
Move the hands, arms, and legs in strange, purposeless ways
Utter meaningless sounds
Not understand what other people are saying
Resist help
Turn the head or eyes toward the side opposite from the seizure focus
Some people can converse, but their conversation lacks spontaneity, and the content is somewhat sparse. They may be confused and disoriented. This state may last for several minutes. Occasionally, people lash out if they are restrained.
Generalized-onset seizures
In generalized-onset seizures, the seizure begins in both sides of the brain. Most generalized-onset seizures impair awareness. They often cause loss of consciousness and abnormal movements, usually immediately. Loss of consciousness may be brief or last a long time.
Generalized-onset seizures include the following types:
Tonic-clonic seizures (formerly, called grand mal seizures; involving initial muscle stiffening followed by rhythmic jerking of muscles)
Clonic seizures (involving sustained rhythmic jerking of muscles after brief initial muscle stiffening)
Tonic seizures (involving stiffening of muscles in all limbs)
Atonic seizures (involving loss of muscle tone)
Myoclonic seizures (involving rhythmic jerking of muscles not preceded by stiffening of muscles and without loss of consciousness)
Myoclonic-tonic-clonic seizures (involving jerking of muscles followed by muscle stiffening and repeated jerking of muscles), including juvenile myoclonic epilepsy
Negative myoclonic seizures (involving repeated very brief loss of muscle tone without muscle contraction)
Myoclonic-atonic seizures (involving jerking of muscles, followed by loss of muscle tone)
Epileptic (infantile) spasms
Absence seizures
Most types of generalized seizures (such as tonic-clonic seizures) involve abnormal muscle contractions. Those that do not are called absence seizures or generalized-onset nonmotor seizures.
Generalized-onset seizures begin with abnormal discharges in a deep, central part of the brain and spread simultaneously to both sides of the brain. There is no aura. The seizure typically begins with an outcry. People then become unaware or lose consciousness.
During generalized-onset seizures, particularly generalized tonic-clonic seizures, people may do the following:
Have severe muscle spasms and jerking throughout the body as muscles rapidly and repeatedly contract and relax
Fall down
Clench their teeth
Bite their tongue (often occurs)
Drool or froth at the mouth
Lose control of the bladder and/or bowels
The seizures usually last 1 to 2 minutes. Afterward, some people have a headache, are temporarily confused, and feel extremely tired. These symptoms may last from minutes to hours. Most people do not remember what happened during the seizure.
In generalized tonic-clonic seizures, muscles contract (the tonic part), then rapidly alternate between contracting and relaxing (the clonic part). These seizures may be
Generalized-onset (starting in both sides of the brain)
Focal to bilateral (starting in 1 side of the brain and spreading to both sides)
In both types, consciousness is temporarily lost and a convulsion occurs when the abnormal discharges spread to both sides of the brain.
Focal-to-bilateral tonic-clonic (grand mal) seizures usually begin with an abnormal electrical discharge in a small area of 1 side of the brain, resulting in a focal preserved-consciousness or focal impaired-consciousness seizure. The discharge then quickly spreads to both sides of the brain, causing the entire brain to malfunction. Symptoms are similar to those of generalized-onset seizures.
Atonic seizures occur primarily in children. They are characterized by a brief but complete loss of muscle tone and consciousness. They cause children to fall to the ground, sometimes resulting in injury.
In clonic seizures, the limbs on both sides of the body and often head, neck, face, and trunk jerk rhythmically throughout the seizure. Clonic seizures usually occur in infants. They are much less common than tonic-clonic seizures.
Tonic seizures occur commonly during sleep, usually in children. Muscle tone increases abruptly or gradually, causing muscles to stiffen. The limbs and neck are often affected. Tonic seizures typically last only 10 to 15 seconds but can cause children, if standing, to fall to the ground. Most children do not lose consciousness. If seizures last longer, muscles may jerk a few times as the seizure ends.
Atypical absence seizures (see below), atonic seizures, and tonic seizures usually occur as part of a severe form of epilepsy called Lennox-Gastaut syndrome, which begins before children are 4 years old.
Myoclonic seizures are characterized by quick sharp jerks of 1 or several limbs or the trunk. The seizures are brief and do not cause loss of consciousness, but they may occur repetitively and may progress to a tonic-clonic seizure with loss of consciousness.
Negative myoclonic seizures are characterized by repeated, abrupt, brief interruption of muscle tone without evidence of myoclonic seizures. The seizures interfere with motor coordination and may cause falls or dropping of objects from the hands.
In myoclonic-atonic seizures, the limbs or trunk jerks briefly, then goes limp (drop attack). Seizures usually begin between the ages of 6 months to 6 years. Before the first myoclonic-atonic seizure, two-thirds of children have febrile seizures and generalized-onset convulsive seizures. Development and mental processes are typically normal, but during or after the seizure, development and thinking may be impaired.
Juvenile myoclonic epilepsy typically begins during adolescence. Typically, seizures begin with quick myoclonic jerks of both arms. About 90% of these seizures are followed by generalized tonic-clonic seizures. Some people also have absence seizures. The seizures often occur when people awaken in the morning, especially if they are sleep-deprived. Drinking alcohol also makes these seizures more likely.
Absence seizures do not involve abnormal muscle contraction. They may be classified as
Typical (formerly called petit mal)
Atypical
Typical absence seizures usually begin in childhood, usually between the ages of 5 and 15 years, and do not continue into adulthood. However, adults occasionally have typical absence seizures. Unlike tonic-clonic seizures, absence seizures do not cause convulsions or other dramatic symptoms. People do not fall down, collapse, or move jerkily. Instead, they have episodes of staring with fluttering eyelids and sometimes twitching facial muscles. They typically lose consciousness, becoming completely unaware of their surroundings. These episodes last 10 to 30 seconds. People abruptly stop what they are doing and resume it just as abruptly. They experience no after-effects and do not know that a seizure has occurred. Without treatment, many people have several seizures a day. Seizures often occur when people are sitting quietly. Seizures rarely occur during exercise. Hyperventilation can trigger a seizure.
Atypical absence seizures differ from typical absence seizures as follows:
They are less common.
They last longer.
Muscle jerks and other movements, such as muscle stiffening and mouth and facial movements, can be seen.
People are more aware of their surroundings.
Most people with atypical absence seizures have neurologic abnormalities or developmental delays. Atypical absence seizures usually continue into adulthood.
Status epilepticus
Convulsive status epilepticus is the most serious seizure disorder and is considered a medical emergency because the seizure does not stop. Electrical discharges occur throughout the brain, causing a generalized tonic-clonic seizure.
Convulsive status epilepticus is diagnosed when 1 or both of the following occur:
A seizure lasts more than 5 minutes
People do not completely regain consciousness between 2 or more seizures
People have convulsions with intense muscle contractions and often cannot breathe adequately. Body temperature increases. Without rapid treatment, the heart and brain can become overtaxed and permanently damaged, sometimes resulting in death.
Generalized convulsive status epilepticus has many causes, including injuring the head and abruptly stopping an antiseizure medication.
Nonconvulsive status epilepticus, another type of status epilepticus, does not cause convulsions. The seizures last 10 minutes or more. During the seizure, mental processes (including awareness) and/or behavior are affected. People may appear confused or spaced out. They may be unable to speak and may behave irrationally. Having nonconvulsive status epilepticus increases the risk of developing convulsive status epilepticus. This type of seizure requires prompt diagnosis and treatment.
Dravet syndrome
Dravet syndrome (severe myoclonic epilepsy of infancy) develops during early childhood. It has focal and generalized characteristics. During the first year of life, focal seizures are typically triggered by fever. At about age 2 years, children tend to have generalized myoclonic seizures. In these seizures, the trunk or 1 or several limbs jerk. Children with Dravet syndrome may also develop other types of seizures.
During the second year of life, children no longer develop as expected and may lose the developmental skills they have achieved. Children have difficulty thinking and learning. They also lack coordination and balance.
In many children with Dravet syndrome, the cause is an abnormal gene known to cause seizures.
Symptoms after a seizure
When a seizure stops, people may have a headache, sore muscles, unusual sensations, confusion, and profound fatigue. These after-effects are called the postictal state. In some people, 1 side of the body is weak after a seizure, and the weakness lasts longer than the seizure (a disorder called Todd paralysis).
Most people do not remember what happened during the seizure (a condition called postictal amnesia).
Complications
Seizures may have serious consequences. Intense, rapid muscle contractions can cause injuries, including broken bones. Sudden loss of consciousness can cause serious injury due to falls and accidents. People may have numerous seizures without incurring serious brain damage. However, seizures that recur and cause convulsions may eventually impair intelligence.
If seizures are not well-controlled, people may be unable to get a driver’s license. They may have difficulty keeping a job or getting insurance. They may be socially stigmatized. As a result, their quality of life may be substantially reduced.
If seizures are not completely controlled, the risk of death is 2 to 3 times higher than for people who do not have seizures.
A few people die suddenly for no apparent reason—a complication called sudden unexpected death in epilepsy. This disorder usually occurs at night or during sleep. Risk is highest for people who have frequent seizures, especially generalized tonic-clonic seizures.
Did You Know...
|
Diagnosis of Seizure Disorders
A doctor's evaluation
If the person has never had a seizure before, blood and other tests, imaging of the brain, and electroencephalography
If a seizure disorder has already been diagnosed and the person is taking medication to prevent seizures, blood tests to measure levels of antiseizure medications
The diagnosis of a seizure is based on symptoms and the observations of eyewitnesses. Symptoms that suggest a seizure include loss of consciousness, muscle spasms that shake the body, a bitten tongue, loss of bladder control, sudden confusion, and inability to pay attention. Doctors diagnose a seizure disorder (epilepsy) when people have at least 2 unprovoked seizures that occur at different times.
People who lose consciousness, sometimes even when they lose muscle tone and muscles jerk, may not be having a seizure. A brief loss of consciousness is more likely to be fainting (syncope) than a seizure.
People with new seizures are usually evaluated in an emergency department. If a seizure disorder has already been diagnosed and people have completely recovered, they may be evaluated in a doctor’s office.
History and physical examination
An eyewitness report of the episode can be very helpful to doctors. An eyewitness can describe exactly what happened, whereas people who have an episode usually cannot. Doctors need to have an accurate description, including the following:
How fast the episode started
Whether it involved abnormal muscle movements (such as spasms of the head, neck, or facial muscles), tongue biting, drooling, loss of bladder or bowel control, or muscle stiffening
How long it lasted
How quickly the person recovered
A quick recovery suggests fainting rather than a seizure. Confusion that lasts for many minutes to hours after consciousness is regained suggests a seizure.
Although eyewitnesses may be too frightened during the seizure to remember all details, whatever they can remember can help. If possible, how long a seizure lasts should be timed with a watch or other device. Seizures that last only 1 or 2 minutes can seem to go on forever.
Doctors also need to know what people experienced before the episode: whether they had a premonition or warning that something unusual was about to happen and whether anything, such as certain sounds or flashing lights, seemed to trigger the episode.
Doctors ask people about possible causes of seizures, such as the following:
Whether people have had a disorder that can cause seizures (such as a brain infection) or a head injury
Which medications or illicit drugs they are using or have recently stopped
Whether they are consuming alcohol or have recently stopped
For people who are taking medications to control seizures, whether they are taking the medications as directed
Whether they are getting enough sleep (not getting enough sleep can make seizures more likely to occur in some people)
With children, whether they have relatives who also have seizures
A thorough physical examination is done. It may provide clues to the cause of the symptoms.
Testing
Once a seizure is diagnosed, more tests are usually needed to identify the cause.
People known to have a seizure disorder may not need tests, except for a blood test to measure the levels of the antiseizure medications they are taking. However, if they have new symptoms or a new event or disorder (such as a head injury or an infection), more tests are done.
Blood tests are done to check for possible causes in someone with a new seizure or abnormal findings on examination. These tests include measurement of blood levels of substances such as sugar, calcium, sodium, and magnesium and tests to determine whether the liver and kidneys are functioning normally. A sample of urine may be analyzed to check for illicit drugs that may not be reported. Such drugs can trigger a seizure.
Electrocardiography may be done to check for an abnormal heart rhythm. Because an abnormal heart rhythm can greatly reduce blood flow (and therefore oxygen supply) to the brain, it can trigger loss of consciousness and occasionally a seizure or symptoms that resemble a seizure.
Imaging of the brain is usually done promptly to check for bleeding or a stroke. Typically, computed tomography (CT) is done, but magnetic resonance imaging (MRI) may be done. Both tests can identify brain abnormalities that could be causing seizures. MRI provides clearer, more detailed images of the brain tissue, but it is not always readily available.
If doctors suspect a brain infection such as meningitis or encephalitis, a spinal tap (lumbar puncture) is done.
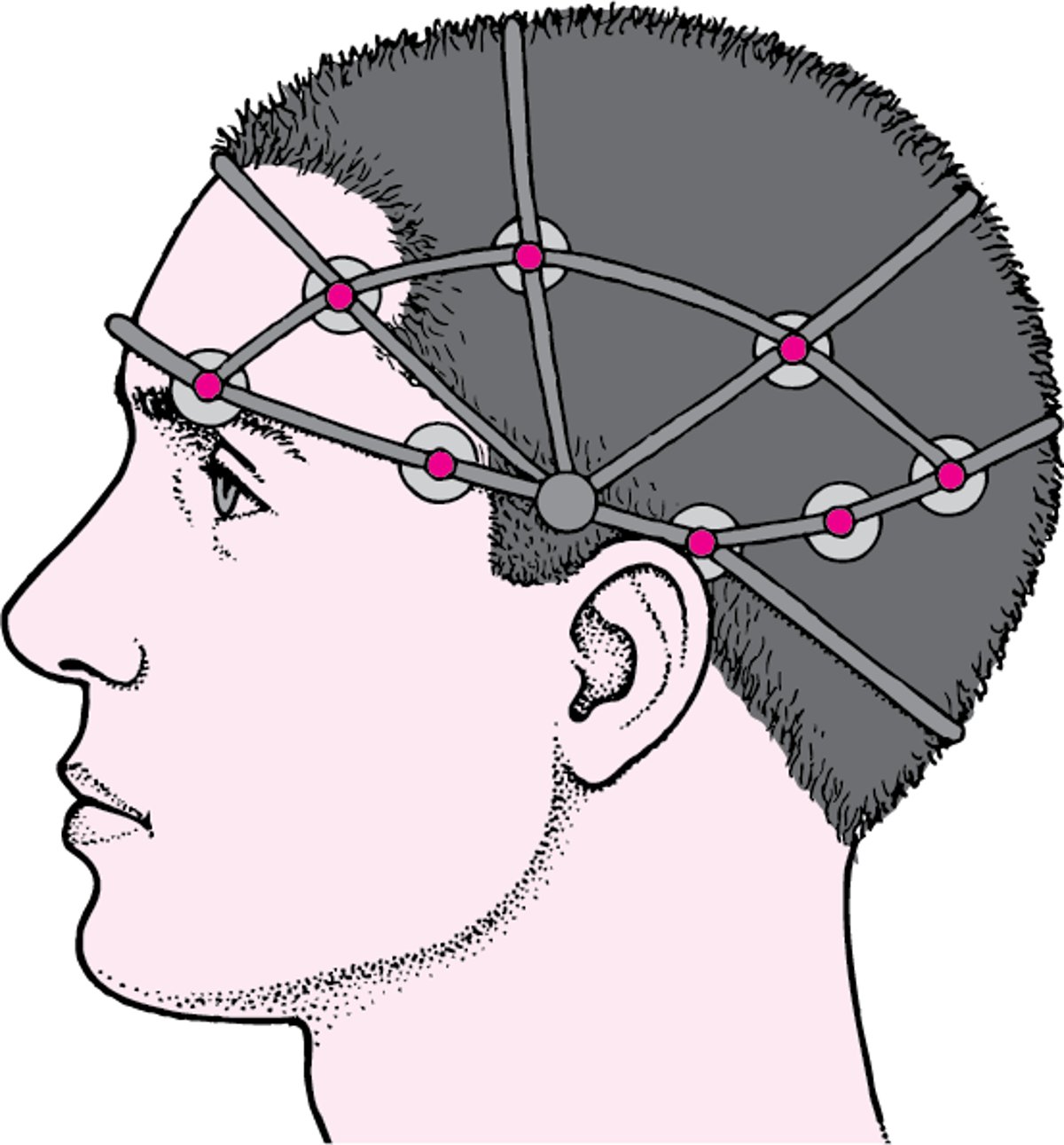
Electroencephalography (EEG) can help confirm the diagnosis. EEG is a painless, safe procedure that records electrical activity in the brain. Doctors examine the recording (electroencephalogram) for evidence of abnormal electrical discharges. Because the recording time is limited, EEG can miss abnormalities, and results may be normal, even in people who have a seizure disorder. EEG may need to be repeated a few times if the initial study was normal. EEG is sometimes scheduled after people have been deprived of sleep for 18 to 24 hours because lack of sleep makes abnormal discharges more likely to occur.
Brain Activity During a Seizure
An electroencephalogram (an EEG) is a recording of the brain’s electrical activity. The procedure is simple and painless. About 20 small adhesive electrodes are placed on the scalp, and the brain’s activity is recorded under normal conditions. Then the person is exposed to various stimuli, such as bright or flashing lights, to try to provoke a seizure. During a seizure, electrical activity in the brain accelerates, producing a jagged wave pattern. Such recordings of brain waves help identify a seizure disorder. Different types of seizures have different wave patterns. | |



If the diagnosis is still uncertain, specialized tests, such as video-EEG monitoring, can be done at an epilepsy center.
For video-EEG monitoring, people are admitted to a hospital for 2 to 7 days, and EEG is done while they are videotaped. If people are taking an antiseizure medication, it is often stopped to increase the likelihood of a seizure. If a seizure occurs, doctors compare the EEG recording with the video recording of the seizure. They may then be able to identify the type of seizure and the area of the brain where the seizure began.
Ambulatory EEG enables doctors to record brain activity for days at a time—while people are at home. It may be useful if seizures recur in people who cannot be admitted to the hospital for a long time.
Treatment of Seizure Disorders
Elimination of the cause if possible
General measures to assure safety and avoid seizure triggers
Medications to control seizures
Sometimes surgery or other procedures if medications are ineffective
If the cause of the seizures can be identified and eliminated, no additional treatment is necessary. For example, if a low blood sugar (glucose) level (hypoglycemia) caused the seizure, glucose is given, and the disorder causing the low glucose level is treated. Other treatable causes include an infection, certain tumors, and an abnormal sodium level.
If the cause cannot be eliminated, general measures plus medications are usually sufficient to treat seizure disorders. If medications are ineffective, surgery may be recommended.
General measures
Exercise is usually recommended and social activities are encouraged. However, people who have a seizure disorder may have to make some adjustments. For example, they may be advised to do the following:
Not drink alcohol
Avoid cocaine or other illicit drugs (for example, phencyclidine and amphetamines)Avoid cocaine or other illicit drugs (for example, phencyclidine and amphetamines)
Until seizures are controlled (seizure-free for at least 6 months), refrain from activities in which a sudden loss of consciousness could result in serious injury, such as bathing in a bathtub, climbing, swimming, or operating power tools
After seizures are controlled, people can resume activities if adequate precautions are taken. For example, they should swim only when lifeguards are present.
In most states in the United States, laws prohibit people with a seizure disorder from driving until they have been free of seizures for at least 6 months to 1 year.
A family member or close friend and coworkers should be trained to help if a seizure occurs. They should not attempt to put an object (such as a spoon) in the person’s mouth to protect the person’s tongue. Such efforts can do more harm than good. The teeth may be damaged, or the person may bite the helper unintentionally as the jaw muscles contract. However, helpers should do the following during a seizure:
Protect the person from falling
Loosen clothing around the neck
Place a pillow under the head
Roll the person over to 1 side
If a pillow is unavailable, helpers can put their foot or place an item of clothing under the person’s head.
People who lose consciousness should be rolled onto one side to ease breathing and prevent them from inhaling vomit or saliva. Inhaling vomit or saliva can lead to aspiration pneumonia (a lung infection caused by inhaling saliva, stomach contents, or both).
People who have had a seizure should not be left alone until they have awakened completely, are no longer confused, and can move about normally. Usually, their doctor should be notified.
Did You Know...
|
Antiseizure medications
Antiseizure medications (also called anticonvulsants or antiepileptic medications) reduce the risk of having another seizure. Usually, they are prescribed only if people have had more than 1 seizure and if no reversible cause of seizure (such as low blood sugar) has been identified. Antiseizure medications are usually not prescribed when people have had only 1 generalized seizure.
Most antiseizure medications are taken by mouth.
Antiseizure medications can completely stop seizures in about one-third of people who have them and greatly reduce the frequency of seizures in another third. Almost two-thirds of people who respond to antiseizure medications can eventually stop taking them without having a relapse. If antiseizure medications are ineffective, people are referred to a seizure center and evaluated for surgery.
There are many different types of antiseizure medications. Which one is effective depends on the type of seizure and other factors. For most people, taking 1 antiseizure medication, usually the first or second one tried, controls seizures. If seizures recur, different antiseizure medications are tried. In such cases, determining which medication is effective may take several months. Some people have to take several medications, which increases the risk of side effects. Some antiseizure medications are not used alone but only with other antiseizure medications.
Doctors take care to determine the appropriate dose for each person. The best dose is the smallest dose that stops all seizures while having the fewest side effects. Doctors ask people about side effects, then adjust the dose if needed. Sometimes doctors also measure the level of antiseizure medication in the blood.
Antiseizure medications should be taken just as prescribed. People who take medications to control seizures should see a doctor regularly for dose adjustment and should always wear a medical alert bracelet inscribed with the type of seizure disorder and the medication being taken.
Antiseizure medications can interfere with the effectiveness of other medications, and vice versa. Consequently, people should make sure their doctor knows all the medications, supplements, and illicit drugs they are taking before they start taking antiseizure medications. They should also talk to their doctor and possibly their pharmacist before they start taking any other medications, including over-the-counter medications.
After seizures are controlled, people take the antiseizure medication until they have been seizure-free for at least 2 years. Then, under guidance by their doctor, the dose of the medication may be decreased gradually, and the medication eventually stopped. If a seizure recurs after the antiseizure medication is stopped, people may have to take an antiseizure medication indefinitely. If seizures are going to recur, they usually do so within 2 years.
Seizures are more likely to recur in people who have had any of the following:
A seizure disorder since childhood
The need to take more than 1 antiseizure medication
Seizures while taking an antiseizure medication
Abnormal EEG results within the previous year
Structural damage to the brain—for example, by a stroke or tumor
Antiseizure medications, although very effective, may have side effects. Many cause drowsiness, but some may make children hyperactive. For many antiseizure medications, blood tests are done periodically to determine whether the medication is impairing kidney or liver function or reducing the number of blood cells.
Some antiseizure medications (phenobarbital, carbamazepine, and phenytoin) can interact with other medications and make them less effective. These medications include birth control pills, anticoagulants, medications used to treat HIV infection, some chemotherapy medications, and some other antiseizure medications. Some antiseizure medications can lower vitamin D levels, increasing the risk of Some antiseizure medications (phenobarbital, carbamazepine, and phenytoin) can interact with other medications and make them less effective. These medications include birth control pills, anticoagulants, medications used to treat HIV infection, some chemotherapy medications, and some other antiseizure medications. Some antiseizure medications can lower vitamin D levels, increasing the risk ofosteoporosis.
People taking antiseizure medications should be aware of possible side effects and should consult their doctor when side effects occur.
For women who have a seizure disorder and are pregnant, taking an antiseizure medication increases the risk of miscarrying or of having a baby with a birth defect of the spinal cord, spine, or brain (neural tube defect—see table ). However, stopping the antiseizure medication may be more harmful to the woman and the baby. Having a generalized seizure during pregnancy can injure or kill the fetus. Consequently, continuing to take an antiseizure medication is usually recommended (see Seizure Disorders During Pregnancy). Women who are of childbearing age and taking an antiseizure medication should take folate supplements to reduce the risk of having a baby with a birth defect.
Did You Know...
|
Medications Used to Treat Seizures
Medication | Use | Some Side Effects |
|---|---|---|
AcetazolamideAcetazolamide | Absence seizures when other antiseizure medications are ineffective | Kidney stones, dehydration, and chemical imbalances in the blood |
CannabidiolCannabidiol | Dravet syndrome Tonic or atonic seizures in Lennox-Gastaut syndrome* | Drowsiness, liver damage, loss of appetite, fatigue, insomnia, and diarrhea |
CarbamazepineCarbamazepine | Focal-onset seizures Secondarily generalized-onset seizures (including focal-to-bilateral tonic-clonic seizures) | A low white blood cell count (neutropenia), production of too few blood cells (aplastic anemia, which can be fatal), a low platelet count (thrombocytopenia), a severe rash, digestive upset, liver damage, slurred speech (dysarthria), lethargy, dizziness, and double vision |
CenobamateCenobamate | Focal-onset seizures with or without focal-to-bilateral tonic-clonic seizures† | Dizziness, double vision, sleepiness, fatigue and, rarely, suicidal thoughts |
ClobazamClobazam | Absence seizures Dravet syndrome Focal-onset or focal-to-bilateral tonic-clonic seizures† when other antiseizure medications are ineffective Sometimes tonic or atonic seizures in Lennox-Gastaut syndrome* | Drowsiness, constipation, loss of coordination, thoughts of suicide, dependency on the medication, irritability, and difficulty swallowing |
ClonazepamClonazepam | Atonic seizures Atypical absence seizures in Lennox-Gastaut syndrome* Epileptic (infantile) spasms Myoclonic seizures | Drowsiness, abnormal behavior, loss of coordination, and loss of effectiveness of the medication after 1 to 6 months |
Divalproex‡ | Absence seizures Dravet syndrome Epileptic spasms Focal-onset seizures Generalized-onset tonic-clonic seizures Juvenile myoclonic epilepsy Myoclonic seizures Tonic or atonic seizures in Lennox-Gastaut syndrome* | Nausea, vomiting, abdominal pain, diarrhea, temporary drowsiness, shaking (tremor), reversible hair loss, weight gain, and liver damage A somewhat higher risk of spinal cord, spine, or brain birth defects (neural tube defects) than with other antiseizure medications |
EslicarbazepineEslicarbazepine | Focal-onset seizures | Dizziness or shakiness, double or blurred vision, drowsiness, headache, nausea, vomiting, a low sodium level in the blood, thoughts of suicide, and skin reactions, such as rash (sometimes serious) |
EthosuximideEthosuximide | Absence seizures | Nausea, lethargy, dizziness, headache, rash, and a low blood cell count (of all types of blood cells) |
FelbamateFelbamate | Used only when other antiseizure medications are ineffective Atypical absence seizures in Lennox-Gastaut syndrome* Focal-onset seizures | Headache, fatigue, liver failure, and, rarely, aplastic anemia (which can be fatal) |
FenfluramineFenfluramine | Adjunctive treatment (used with another antiseizure medication) for Dravet syndrome | Decreased appetite, fever, diarrhea, fatigue, pharyngitis. |
Fosphenytoin§Fosphenytoin§ | Focal impaired-awareness seizures Status epilepticus Focal-to-bilateral tonic-clonic seizures† Prevention of seizures after a head injury | Loss of coordination, drowsiness, dizziness, headache, itching, and tingling sensations |
GabapentinGabapentin | Adjunctive treatment (used with another antiseizure medication) for:
| Drowsiness, dizziness, weight gain, and headache In children, sleepiness, aggressive behavior, mood swings, and hyperactivity |
LacosamideLacosamide | Focal-onset seizures Generalized tonic-clonic seizures in people 4 years or older | Dizziness, double vision, and thoughts of suicide |
LamotrigineLamotrigine | Adjunctive treatment for:
| Nausea, vomiting, constipation, headache, drowsiness, dizziness, insomnia, fatigue, loss of coordination, double vision, tremor, abnormal menstrual periods, and rash |
LevetiracetamLevetiracetam | Status epilepticus Adjunctive treatment for:
| Dizziness, weakness, fatigue, loss of coordination, and changes in mood and behavior |
OxcarbazepineOxcarbazepine | Focal-onset seizures | Headache, abdominal pain, double vision, drowsiness, dizziness, fatigue, nausea, and low sodium levels in the blood |
PerampanelPerampanel | Adjunctive treatment for:
| Aggressiveness, changes in mood and behavior, thoughts of suicide, dizziness, fatigue, irritability, falls, sleepiness, nausea, vomiting, headache, weight gain, abdominal pain, and problems walking |
PhenobarbitalPhenobarbital | Focal-onset seizures Generalized-onset tonic-clonic seizures Neonatal seizures Status epilepticus | Drowsiness, abnormal eye movements (nystagmus), loss of coordination, anemia, and rash In children, hyperactivity and learning difficulties |
Phenytoin§Phenytoin§ | Focal impaired-consciousness seizures Focal-to-bilateral tonic-clonic seizures† Status epilepticus (phenytoin is given intravenously)Status epilepticus (phenytoin is given intravenously) Prevention of seizures after a head injury | Swollen gums, a low red blood cell count (anemia), loss of bone density, excessive hairiness (hirsutism), rash, and swollen glands When high doses of phenytoin are given, loss of coordination, slurred speech, abnormal eye movements, lethargy, confusion, drowsiness, nausea, and vomitingWhen high doses of phenytoin are given, loss of coordination, slurred speech, abnormal eye movements, lethargy, confusion, drowsiness, nausea, and vomiting |
PregabalinPregabalin | Adjunctive treatment for focal-onset seizures | Dizziness, drowsiness, loss of coordination, blurred vision, double vision, tremor, and weight gain |
TiagabineTiagabine | Adjunctive treatment for focal-onset seizures | Drowsiness, dizziness, confusion, slow thinking, abdominal pain, fatigue, nausea, and tremor |
TopiramateTopiramate | Atypical absence seizures Dravet syndrome Focal-onset seizures Generalized-onset tonic-clonic seizures | Confusion, reduced concentration, difficulty finding words, fatigue, loss of appetite and weight, numbness or tingling, reduced sweating, and kidney stones |
Valproate‡ | Absence seizures Dravet syndrome Febrile seizures Focal-onset seizures Generalized-onset tonic-clonic seizures Epileptic spasms Juvenile myoclonic epilepsy Myoclonic seizures Neonatal seizures Tonic or atonic seizures in Lennox-Gastaut syndrome* Status epilepticus | Nausea, vomiting, abdominal pain, diarrhea, weight gain, reversible hair loss, temporary drowsiness, tremor, and, rarely, liver damage A somewhat higher risk of spinal cord, spine, or brain birth defects (neural tube defects) than with other antiseizure medications |
VigabatrinVigabatrin | Epileptic spasms Focal-onset seizures | Drowsiness, dizziness, headache, fatigue, and permanent changes in vision |
ZonisamideZonisamide | Focal-onset seizures Dravet syndrome Sometimes tonic or atonic seizures in Lennox-Gastaut syndrome* | Depression, psychosis, kidney stones, reduced sweating |
* Atypical absence seizures, atonic seizures, and tonic seizures usually occur as part of a severe form of epilepsy called Lennox-Gastaut syndrome, which begins before children are 4 years old. | ||
† Focal-to-bilateral seizures are seizures that start on one side of the brain and spread to both sides. | ||
‡ Divalproex and valproate are similar. | ||
§ Fosphenytoin and phenytoin are similar.§ Fosphenytoin and phenytoin are similar. | ||
Emergency treatment
Emergency treatment to stop the seizures is required for
Status epilepticus (seizures that last more than 5 minutes)
Large doses of 1 or more antiseizure medications (often starting with a benzodiazepine, such as lorazepam) are given intravenously as quickly as possible to stop the seizure. The sooner antiseizure medications are started, the more easily seizures are controlled. Large doses of 1 or more antiseizure medications (often starting with a benzodiazepine, such as lorazepam) are given intravenously as quickly as possible to stop the seizure. The sooner antiseizure medications are started, the more easily seizures are controlled.
Measures to prevent injuries are taken during the prolonged seizure. People are monitored closely to make sure breathing is adequate. If it is not, a tube is inserted to help with breathing—a procedure called intubation.
If seizures persist, a general anesthetic is given.
Surgery
If people continue to have seizures while taking 2 or more antiseizure medications or if they cannot tolerate side effects of the medications, brain surgery may be done. These people are tested at specialized epilepsy centers to determine whether surgery can help. Testing may include MRI of the brain, video-EEG monitoring, and the following:
Functional MRI: To determine which areas in the brain are causing seizures (called seizure foci)
Single-photon emission CT (SPECT): To check for areas with increased blood flow around the time of a seizure, which may indicate which areas in the brain are causing seizures
EEG combined with magnets used for imaging (magnetic source imaging): Also to help determine which areas in the brain are causing seizures
If a defect in the brain (such as a scar) can be identified as the cause and is confined to a small area, surgically removing that area can eliminate seizures in up to 60% of people, or surgery may reduce the severity and frequency of seizures.
Surgically cutting the nerve fibers that connect the 2 sides of the brain (corpus callosum) may help people who have seizures that originate in several areas of the brain or that spread to all parts of the brain very quickly. This procedure usually has no appreciable side effects. However, even if surgery reduces the frequency and severity of seizures, many people need to continue to take antiseizure medications, although they can usually take lower doses or fewer medications.
Before and after surgery, a psychological and neurologic evaluation may be done to determine how well the brain is functioning.
If people cannot undergo these surgical procedures, other procedures, such as stimulation of the vagus nerve or brain, may be done.
Stimulation of the vagus nerve
Electrical stimulation of the tenth cranial nerve (vagus nerve) can reduce the number of focal-onset seizures by more than one-half in about 40% of people who have focal-onset seizures. This treatment is used when seizures continue despite use of antiseizure medications and when surgery is not a possibility.
The vagus nerve is thought to have indirect connections to areas of the brain often involved in causing seizures.
For this procedure, a device that looks like a heart pacemaker (vagus nerve stimulator) is implanted under the left collarbone and is connected to the vagus nerve in the neck with a wire that runs under the skin. The device causes a small bulge under the skin. The operation is done on an outpatient basis and takes about 1 to 2 hours.
The device is programmed to periodically stimulate the vagus nerve. Also, people are given a magnet, which they can use to stimulate the vagus nerve when they sense that a seizure is about to begin. Vagus nerve stimulation is used in addition to antiseizure medications.
Side effects of vagal nerve stimulation include hoarseness, cough, and deepening of the voice when the nerve is stimulated.
Stimulation of the brain
The responsive neurostimulation system is a device that looks like a heart pacemaker. It is implanted within the skull. The device is connected by wires to 1 or 2 areas in the brain that are causing the seizures. This system monitors the brain's electrical activity. When it detects unusual electrical activity, it stimulates the areas of the brain that are causing the seizures. The aim is to restore normal electrical activity in the brain before a seizure can occur.
The responsive neurostimulation system is used in addition to antiseizure medications. It is used when adults have focal-onset seizures that are not controlled by medications. It can reduce the frequency of seizures in these people.
Surgery to implant the system requires general anesthesia and typically takes 2 to 4 hours. Many people can go home the next day. Some need to stay in the hospital for up to 3 days. Many people can return to their daily activities within a few days and return to work in 2 to 4 weeks.
People cannot feel the device or the stimulation, and the device can be removed if needed.
Prognosis for Seizure Disorders
With medication, one-third of people with epilepsy are free from seizures, and most become seizure-free shortly after starting treatment. In another third, seizures recur less than half as often as they did before treatment. If seizures are well-controlled with medications, about 60 to 70% of people can eventually stop taking antiseizure medications and remain seizure-free.
Epileptic seizures are considered resolved when people have been seizure-free for 10 years and have not taken antiseizure medications for the last 5 years of that time period.
Drug Information for the Topic


