


Metabolic and bariatric (weight-loss) surgery alters the stomach, intestine, or both to produce weight loss in people have obesity or overweight and have metabolic disorders related to obesity (such as diabetes or abnormal lipid levels) or other weight-related complications (such as high blood pressure, sleep apnea, or heart disease).
In the United States, about 260,000 people have metabolic and bariatric surgery each year. This number accounts for almost two-thirds of the total number of bariatric procedures done worldwide. These procedures result in substantial weight loss. People may lose half or even more of their excess weight and as much as 80 to 160 pounds. Weight loss is rapid at first and then slows gradually over a period of about 1 to 2 years. Weight loss is often maintained for years. The loss greatly reduces the severity and risk of weight-related medical problems (such as sleep apnea and diabetes). It improves mood, self-esteem, body image, activity level, and the ability to work and interact with other people.
Experts in bariatric surgery recommend surgery for people with a body mass index (BMI) of over 35, regardless of other health conditions, and for those with a BMI 30 to 34.9 with metabolic disorders (such as diabetes and heart disease). Many of these people also qualify for weight-loss medications. How to use these medications with surgery is under study.
To qualify for surgery, people also need to do the following:
Understand the risks and effects of metabolic and bariatric surgery
Be motivated to follow the changes in diet and lifestyle required after surgery
Have tried other methods of losing weight
Be physically and mentally able to undergo surgery
Specific testing before surgery and the length of time between referral and surgery can vary based on the person's insurance company.
Usually, age alone is not a factor when metabolic and bariatric surgery is being considered. In people under 18, metabolic and bariatric surgery has had good short- and long-term results.
Surgery is not appropriate if people
Have a mental health disorder that is not under control (such as major depression)
Have a substance use disorder
Have cancer that is not in remission or another life-threatening disorder
Types of Metabolic and Bariatric Surgery
Metabolic and bariatric surgery is done using one of two methods:
Minimally invasive surgery
Open abdominal surgery
Usually, minimally invasive techniques—laparoscopy or robotic-assisted procedures—are used. In laparoscopic procedures, a tube fitted with a camera (laparoscope) is inserted into a small incision near the navel. Four to six other surgical instruments are then inserted into the abdomen through similar small incisions. In robotic-assisted procedures, the surgeon uses robotic arms to hold and manipulate the instruments threaded through the small incisions. Traditional open surgery uses a long incision up and down the middle of the abdomen, and is now performed only in certain cases. Minimally invasive techniques result in less pain and a shorter healing time than open surgery.
Metabolic and bariatric surgery may involve
Reducing the size of the stomach, sometimes bypassing part of the small intestine (for example, the Roux-en-Y gastric bypass)
Endoscopic procedures (such as placement of a balloon in the stomach)
Both of these procedures limit the amount of food people can eat. Also, they result in changes in metabolism and hormones that promote weight loss—for example, by making people feel full sooner.
The most common procedures done in the United States include the following:
Revisional procedures (such as reducing the size of the stomach pouch)
Biliopancreatic diversion with duodenal switch (BPD/DS)
Single anastomosis duodeno-ileal bypass with sleeve gastrectomy
Endoscopic procedures
Some procedures such as the vertical banded gastroplasty and adjustable gastric banding are rarely done now.
Sleeve gastrectomy
Sleeve gastrectomy is the most commonly used metabolic and bariatric surgical procedure in the United States. It causes substantial and sustained weight loss.
Most of the stomach is removed, making the stomach into a narrow tube (sleeve) that resembles a banana. The small intestine is not altered.
The resulting sleeve holds less food and thus reduces the number of calories consumed. People also feel less hungry.
Sleeve gastrectomy results in certain hormonal changes, which may result in feeling full sooner and which may contribute to weight loss. These changes also improve how the body uses glucose, possibly helping reduce the severity of diabetes.
Serious complications are rare. An infection can occur if the stomach contents leak outside of the sleeve. Gastroesophageal reflux disease (GERD) may develop or worsen. People who have significant symptoms due to GERD before surgery may be advised against sleeve gastrectomy. Serious bleeding can occur with any surgical procedure.
Roux-en-Y gastric bypass
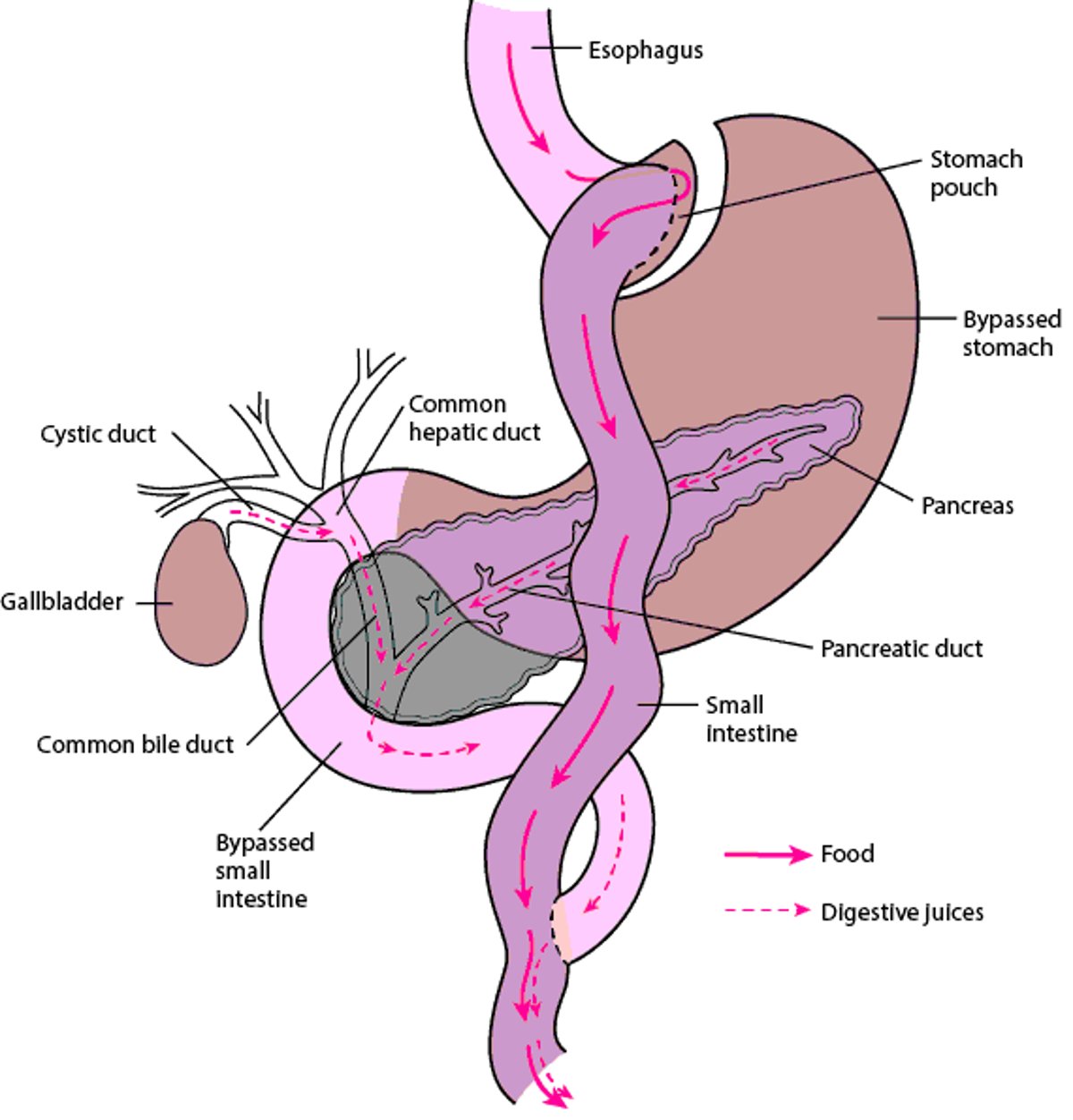
For Roux-en-Y gastric bypass, a small part of the stomach is detached from the rest, creating a small stomach pouch. As a result, the amount of food that can be eaten at one time is drastically reduced. The stomach pouch is connected to a lower part of the small intestine (called the jejunum). Thus, a large part of the stomach and small intestine is bypassed. This arrangement resembles a Y—hence the name. The opening between the pouch and the intestine is made narrow. As a result, food moves slowly out of the pouch into the intestine, and people may feel full for a longer time. Because food bypasses the lower, disconnected part of the stomach and the upper part of the small intestine (duodenum), where much of the digestion and absorption occurs, the amount of food and number of calories absorbed is reduced. The bypassed parts of the stomach and duodenum are then connected lower in the small intestine so that digestive juices (bile acids produced by the liver and pancreatic enzymes) can still mix with food and food can still be digested. Also nutrients, including vitamins and minerals, can still be absorbed, reducing the risk of nutritional deficiencies.
Gastric bypass (and sleeve gastrectomy) results in certain hormonal changes. These changes may result in feeling full sooner and may contribute to weight loss. These changes also improve how the body uses glucose (a sugar), possibly helping reduce the severity of diabetes or causing it to resolve.
Most people stay in the hospital overnight or longer.
For many people who have had a gastric bypass, eating foods high in fat and refined sugar can cause dumping syndrome. Symptoms of dumping syndrome include indigestion, nausea, diarrhea, abdominal pain, sweating, light-headedness, and weakness. Dumping syndrome occurs when undigested food from the stomach moves into the small intestine too quickly. Similar to sleeve gastrectomy, complications of gastric bypass can include infection if the stomach contents leak out of the stomach at the new connections and bleeding. Blockage of the intestine is a rare complication that can occur any time after surgery.
Bypassing Part of the Digestive Tract
For this procedure (called Roux-en-Y gastric bypass), part of the stomach is detached from the rest, creating a small pouch. The pouch is connected to a lower part of the small intestine —an arrangement that resembles a Y. As a result, parts of the stomach and small intestine are bypassed. However, digestive juices (bile acids and pancreatic enzymes) can still mix with food, enabling the body to absorb vitamins and minerals and reducing the risk of nutritional deficiencies. |

Revisional procedures
Sometimes a second (called revisional) procedure is needed when people have not reached their weight goal or have regained the weight they lost, or because a different complication has occurred. For example, if gastroesophageal reflux disease (GERD) develops after sleeve gastrectomy. GERD can be treated by doing a Roux-en-y gastric bypass.
Revisional procedures can be more complicated and have a slightly higher risk of complications than the original surgery. However, these procedures are safe and effective when done by experienced bariatric surgeons.
The type of revisional procedure depends on the original procedure and the reason for the revision. For example if gastric bypass was done, the stomach pouch may stretch and need to be made smaller. Or, surgeons may shorten the part of the small intestine that is attached to the stomach. These procedures reduce the absorption of calories and nutrients and the amount of food a person can eat.
Before a revisional procedure, endoscopy is usually done. A flexible viewing tube is passed through the mouth and down the throat to examine the upper part of the digestive tract. Barium x-ray studies may also done. X-rays are taken after a person swallows barium, which outlines the digestive tract and helps doctors identify abnormalities there.
Biliopancreatic diversion with a duodenal switch
Biliopancreatic diversion with a duodenal switch accounts for fewer than 5% of bariatric procedures done in the United States. However, the number of procedures done each year is increasing.
Biliopancreatic diversion with a duodenal switch is usually done only in people with very severe obesity.
This procedure has three main steps:
Division of the first portion of the small intestine (the duodenum)
Connection between the lower part small intestine (ileum) and the duodenum
An additional connection is made between two parts of the ileum to create a Y similar to that done in the Roux-en-y gastric bypass.
First, a sleeve gastrectomy is done to remove most of the stomach.
The first part of the small intestine (the duodenum) is then divided just after the end of the stomach. The lower part of the intestine (the ileum) is attached to the duodenum so that food goes through the sleeve from the beginning of the duodenum to the ileum. Then, the second connection is made between two parts of the ileum.
Thus, much of the middle part of the small intestine (jejunum) is bypassed. As a result, digestive juices (bile acids and pancreatic enzymes) cannot mix with food where they usually do, and absorption of nutrients and calories is reduced. Weight loss is substantial, but nutritional deficiencies can result if supplements are not taken. After this procedure, doctors do tests to check for vitamin and mineral deficiencies. Biliopancreatic diversion with a duodenal switch may also help people with metabolic syndrome.
Biliopancreatic diversion with a duodenal switch can be done as one or two procedures: first, sleeve gastrectomy alone, then biliopancreatic diversion with duodenal switch after initial weight loss.
Single anastomosis duodeno-ileal bypass with sleeve gastrectomy
Single anastomosis duodeno-ileal bypass with sleeve gastrectomy is similar to biliopancreatic diversion with a duodenal switch but is slightly simpler and faster, and the risk of nutritional deficiencies is less because the part of the small intestine that absorbs nutrients is longer. The main difference is that single anastomosis duodeno-ileal bypass with sleeve gastrectomy involves only one connection.
First, a sleeve gastrectomy is done to remove a large part of the stomach, and the smaller banana-shaped stomach is formed.
Then, the first part of the small intestine (duodenum) is cut just below the stomach. Another cut is made several feet from the lower end of the small intestine (ileum). The cut end of the duodenum attached to the stomach is then connected to the ileum. Because the length of this new segment of small intestine remains relatively long, more nutrients are absorbed.
After this procedure, people must still take nutritional supplements and be monitored for deficiencies, although they less likely to occur than after the biliopancreatic diversion with duodenal switch. Weight loss is substantial and maintained, people feel less hungry, and blood sugar is controlled.
This procedure may worsen or lead to gastroesophageal reflux symptoms. Bile reflux can also occur.
Endoscopic procedures
New endoscopic procedures can help treat people who are not able to have surgery or who prefer not to have surgery.
In one procedure, an uninflated balloon is passed down the throat into the stomach and is filled with saline. The balloon reduces the amount of food that the stomach can hold so that people feel full after eating a smaller amount of food. After 6 months, the balloon is removed. People lose weight initially, but over the long term, they may gain the weight back.
Another procedure is endoscopic sleeve gastroplasty. A doctor inserts an endoscope through the mouth down the throat into the stomach and threads instruments through the endoscope and into the stomach. The doctor then stitches the stomach from within to make the stomach smaller. Complication rates are low. The most common complications include nausea, gastrointestinal bleeding, leaking of the stomach contents, and infections.
Gastroesophageal reflux is less likely to occur after endoscopic sleeve gastroplasty. Also, endoscopic sleeve gastroplasty may be reversible. Results after 5 years suggest weight loss is maintained, However, although some people require revisional procedures.
Adjustable gastric banding
Adjustable gastric banding is now rarely used in the United States. More often, people who have had this procedure have the bands removed and have a sleeve gastrectomy or gastric bypass done.
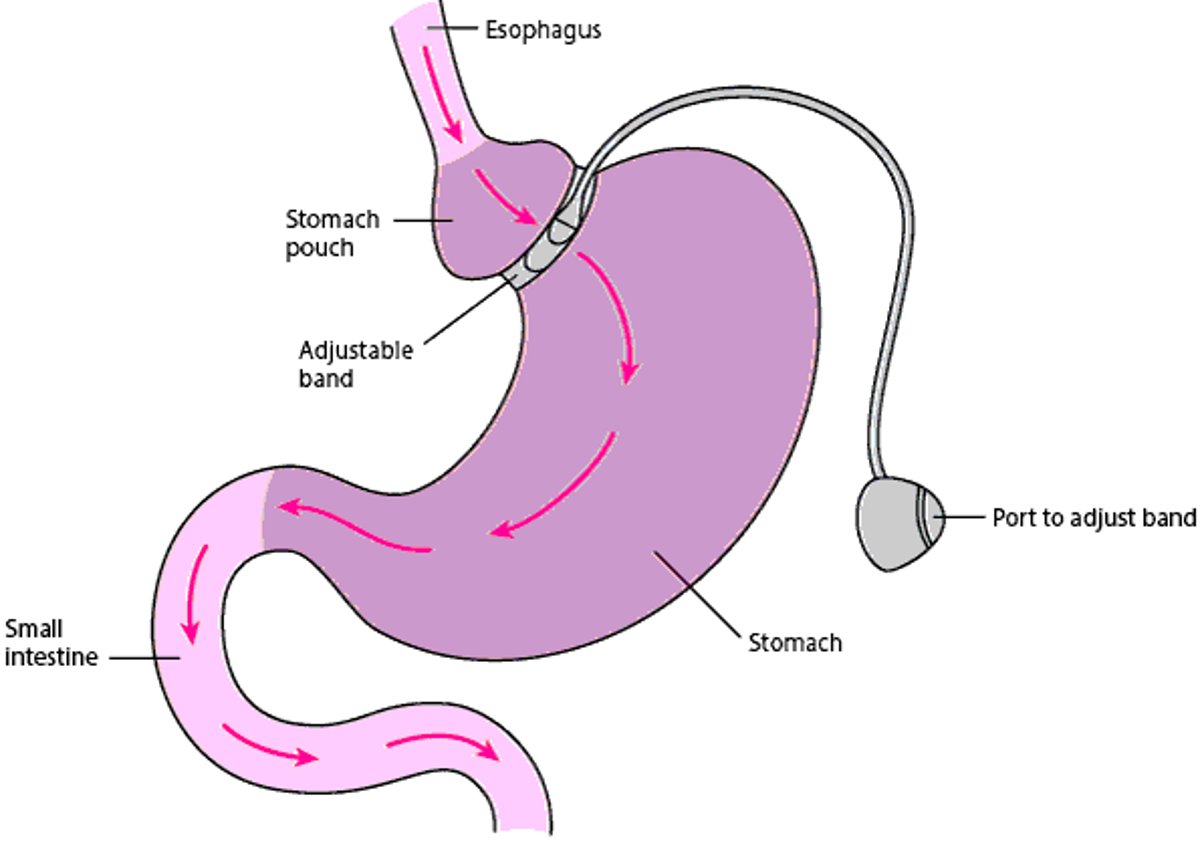
For adjustable gastric banding, a band is placed at the upper end of the stomach to divide the stomach into a small upper part and a large lower part. Food passes through the band on its way to the intestine, but the band slows the passage of food. Connected to the band is a piece of tubing with a device that allows access to the band at the other end of the tube (through a port). The port is placed just under the skin so that doctors can adjust the tightness of the band after surgery. Doctors can inject fluid through the port into the band to expand it and make the passageway between the upper and lower stomach smaller. Or they can remove fluid from the band to make the passageway larger if a problem occurs or the band is too restrictive. When the passageway is smaller, the upper part of the stomach fills more quickly, sending a message to the brain that the stomach is full. As a result, people eat smaller meals and lose substantial amounts of weight over time.
Over the long term, complications include gastroesophageal reflux, esophagitis, slipped bands, and deterioration of tissue under the band.
Banding the Stomach
For this procedure, an adjustable band is placed around the upper part of the stomach. It enables doctors to adjust the size of the passageway for food through the stomach as needed. After a small incision is made in the abdomen, a viewing tube (laparoscope) is inserted. While looking through the laparoscope, the surgeon places the band around the upper part of the stomach. On the inside of the band is an inflatable ring, which is connected to tubing with a small port at the other end. The port is placed just under the skin. A special needle can be inserted into the port through the skin. The needle is used to insert a salt water (saline) solution into the band or to remove the saline. Thus, the passageway can be made smaller or larger. When the passageway is smaller, the upper part of the stomach fills faster, causing people to feel full more quickly and thus eat less. |

Evaluation for Metabolic and Bariatric Surgery
Before metabolic and bariatric surgery, people are evaluated to determine whether surgery is likely to help them. Doctors try to determine how ready and able people are to follow the lifestyle changes required after the surgery.
A physical examination and tests are done. Tests may include the following:
Tests that are routinely done before surgery to check how well vital organs are functioning
Blood tests, including liver tests (to determine how well the liver is functioning and whether it is damaged) and measurement of blood sugar levels and cholesterol and other fat (lipid) levels (after fasting)
Blood tests to measure vitamin D, vitamin B12, folate, and iron levels
Electrocardiography to check for coronary artery disease
Sometimes evaluation of the digestive tract (with x-rays or endoscopy)
Sometimes ultrasonography of the abdomen, including the gallbladder
Sometimes echocardiography (ultrasonography of the heart)
Sometimes pulmonary function tests to evaluate how well the lungs are functioning—for example, if people have asthma or chronic obstructive pulmonary disease (COPD)
Sometimes thyroid function tests
Sometimes sleep evaluation (including polysomnography) and testing for sleep apnea
When certain disorders are detected, measures are taken to control them and thus reduce the risk of surgery. For example, high blood pressure is treated. People who smoke are advised to stop at least 8 weeks before surgery and preferably permanently. Smoking increases the risk of respiratory problems and the risk of ulcers and bleeding in the digestive tract after surgery.
After Metabolic and Bariatric Surgery
After surgery, pain relievers are prescribed.
After metabolic and bariatric surgery, some symptoms are common and do not indicate a problem. However, the following symptoms require a call or visit to the doctor:
Signs of infection at the incision site, such as redness, severe pain, swelling, a bad odor, or oozing
Separation of stitched edges of the incision
Continued or increasing abdominal pain
Persistent fever or chills
Vomiting
Persistent bleeding from the incision site
Abnormal beating of the heart
Diarrhea
Dark, tarry, foul-smelling stools
Shortness of breath
Sweating
Sudden paleness
Chest pain
How quickly people can return to a normal diet varies. For about the first 2 weeks, the diet is mostly liquids. People are asked to drink small amounts frequently throughout the day. They should drink as much fluid as prescribed. Most of the fluid should be a liquid protein supplement. For the next 2 weeks, people should consume a soft diet consisting mostly of mashed or pureed high-protein foods and protein supplements. After 4 weeks, they can usually start eating solid foods.
The following can help people avoid digestive problems and discomfort:
Taking small bites of food
Chewing food thoroughly
Avoiding high-fat and high-sugar foods, such as fast food, cakes, and cookies
Eating only small amounts at each meal
Avoiding drinking liquids when eating solid foods
Adjusting to new eating patterns can be difficult. People may benefit from counseling and/or support groups.
Usually, people can resume taking their routine medications after surgery. But tablets may have to be crushed, and if people have been taking long-acting or sustained-release formulations of medications, doctors must switch them to immediate-release formulations.
People should start walking or doing leg exercises the day after surgery. To avoid blood clots, they should not stay in bed for long periods of time. They can return to their usual activities after about 1 week and to their usual exercises (such as aerobics and strength training) after a few weeks. They should consult their doctor before doing any heavy lifting and manual labor, which should usually be avoided for 6 weeks.
Possible problems
People may experience pain, and some have nausea and vomiting. Constipation is common. Drinking more fluids and not staying in bed too long at a time can help relieve constipation.
Serious complications, such as problems with the incision, infections, blood clots that travel to the lungs (pulmonary embolism), and lung problems, can occur after any operation (see After Surgery).
In addition, the following complications can occur after metabolic and bariatric surgery:
Blockage of the intestine: In about 2 to 4% of people, the intestine becomes blocked because it becomes twisted or scar tissue forms. A blockage can develop weeks to months to years after surgery. Symptoms include severe abdominal pain, nausea, vomiting, difficulty passing gas, and constipation.
Leakage: In about 1 to 3% of people, the new connection between the stomach and intestine leaks. Leakage usually occurs within 2 weeks of surgery. As a result, the stomach’s contents can leak into the abdominal cavity (peritoneum) and cause a serious infection (peritonitis). Symptoms include a fast heart rate, abdominal pain, fever, shortness of breath, and a general sick feeling.
Bleeding: Bleeding may occur at the connection between the stomach and intestine, elsewhere in the digestive tract, or in the abdominal cavity. People may vomit blood or have bloody diarrhea or dark, tarry stools.
Gallstones: Many people who successfully follow a diet aimed at quick weight loss develop gallstones. Up to 15% of people who have metabolic and bariatric surgery need to have their gallbladder removed later.
Kidney stones: Roux-en-Y gastric bypass slightly increases the risk of kidney stones because oxalate accumulates in urine. A high level of oxalate in the urine contributes to calcium stone formation. To prevent stones from forming, people are advised to avoid eating foods that contain oxalate after this surgery. Foods that are high in oxalate include spinach, rhubarb, almonds, baked potatoes with the skin, corn grits, and soy flour.
Gout: Obesity increases the risk of developing gout. In people with gout, gout attacks may occur more frequently after metabolic and bariatric surgery.
Nutritional deficiencies: If people do not make a concentrated effort to eat enough protein, a protein deficiency may develop. Vitamins and minerals (such as vitamins B12 and D, calcium, and iron) may not be absorbed as well after the surgery. Thiamin deficiency can occur if vomiting continues for a long time. People need to take vitamin supplements and sometimes mineral or other supplements (depending on the type of surgery) for the rest of their life.
Reproductive health: Fertility in women of reproductive age may improve after surgery. These women should consider contraceptive choices before and after bariatric procedures, avoid pregnancy prior to surgery, and avoid pregnancy for 12 to 18 months after surgery.
Death: In specially accredited hospitals, the mortality rate is 0.2 to 0.3% during the first month after surgery. The risk of death (and serious complications) may be higher at other hospitals. Causes of death include a blood clot that travels to the lungs, a severe infection due to leakage of one of the connections in the stomach or intestine, a heart attack, pneumonia, and blockage of the small intestine. Risk is higher for people who have had blood clots or obstructive sleep apnea and for people who were not functioning well before surgery or require open surgery. Having very severe obesity or being male or older may increase the risk of death.
Weight loss
Average weight loss after metabolic and bariatric surgery depends on the procedure. Weight loss is usually described as a percentage of excess weight lost. Excess weight is defined as the difference between a person's actual and ideal weight.
For sleeve gastrectomy, loss of excess weight is 33 to 58% after 2 years.
For Roux-en-Y gastric bypass, loss of excess weight is 50 to 65% after 2 years.
For BPD-DS and SADI-S, people lose 75 to 90% of excess body weight.
Although most people gain some weight back, most weight loss can be maintained for up to 10 years.
Follow-up
Visits to the doctor are usually scheduled every 4 to 12 weeks during the first several months after Roux-en-Y gastric bypass or sleeve gastrectomy—the time when weight loss is most rapid. Then visits are scheduled every 6 to 12 months.
At these visits, weight and blood pressure are measured, and eating habits are discussed. People should report any problems they are having. Blood tests are done at regular intervals. Bone density may be measured to check for bone loss due to vitamin D deficiency.
Doctors also check whether people are responding differently to certain medications after surgery. These medications include those used to treat high blood pressure (antihypertensives), diabeteslipid-lowering medications). After surgery, these medications may be stopped completely after weight is lost and these disorders become less severe.
Other benefits
Many disorders that were present before surgery tend to resolve or become less severe after metabolic and bariatric surgery. These disorders include some heart problems, diabetes, obstructive sleep apnea, arthritis, and depression. Diabetes resolves in up to 62% of people 6 years after Roux-en-Y gastric bypass.
Risk of death decreases by 25%, mainly because risk of death due to heart disorders or cancer is reduced.






