




Injury is the number one cause of death for people aged 1 to 44. In the US, there were 278,345 trauma deaths in 2020, about 70% of which were accidental. Of intentional injury deaths, more than 65% were due to self-harm. In addition to deaths, injury results in about 37.9 million emergency department visits and 2.6 million hospital admissions annually.
Patients whose injuries are serious but not immediately fatal benefit the most from treatment in designated trauma centers, hospitals that have special staffing and protocols to provide immediate care to critically injured patients. Criteria for such designation (and for the necessity of transport to them) vary by state but usually follow the guidelines of the American College of Surgeons Committee on Trauma.
Many traumatic injuries are discussed elsewhere in THE MANUAL:
Etiology
Of the myriad ways people are injured, most can be categorized as blunt or penetrating. Blunt injury involves a forceful impact (eg, blow, kick, strike with an object, fall, motor vehicle crash, blast). Penetrating injury involves breach of the skin by an object (eg, knife, broken glass) or projectile (eg, bullet, shrapnel from an explosion).
Other injury types include thermal and chemical burns, toxic inhalations or ingestions, and radiation injury.
Pathophysiology
All injuries, by definition, cause direct tissue damage, the nature and extent depending on the anatomic site, mechanism, and intensity of trauma. Severe direct tissue damage to critical organs (eg, to the heart, brain, spinal cord) is responsible for most immediate trauma deaths.
Additionally, patients surviving the initial insult may develop subsequent indirect injuries in the short and near term. Disruption of blood vessels causes hemorrhage, which may be external (and hence visible) or internal, either confined within an organ as a contusion or hematoma, or as free hemorrhage into a body compartment (eg, peritoneal cavity, thorax). Small amounts of hemorrhage (ie, < 10% of blood volume) are tolerated well by most patients. Larger amounts cause progressive declines in blood pressure and organ perfusion (shock), leading to cellular dysfunction, organ failure, and eventually death. Hemorrhagic shock and brain injury cause most short-term (ie, within hours) deaths, and multiple organ failure due to prolonged shock causes many of the near-term (ie, first 14 days) deaths. Additional near-term deaths result from infection because of disruption of normal anatomic barriers and immune system dysfunction.
Evaluation and Treatment
Primary survey: A, B, C, D, E evaluation and stabilization of Airway, Breathing, Circulation, Disability (neurologic status), and Exposure/Environmental control
Secondary survey: Head-to-toe examination after initial stabilization
Selective use of CT and other imaging studies
Care in the emergency department rather than emergency care delivered at the accident site is discussed here. Evaluation and treatment are done simultaneously, beginning with systems that pose the most immediate threat to life if damaged. Attending to dramatic but not deadly injuries (eg, open lower-extremity fracture, finger amputations) before evaluating immediate life threats can be a fatal mistake. A helpful mnemonic is A, B, C, D, E, for Airway, Breathing, Circulation, Disability (neurologic status), and Exposure/Environmental control. Systems are rapidly examined for serious abnormalities (primary survey); a more detailed examination (secondary survey) is done after the patient is stable.
Pearls & Pitfalls
|
Airway
Airway patency is threatened by blood clots, teeth, or foreign bodies in the oropharynx; soft-tissue laxity and posterior retraction of the tongue caused by obtundation (eg, due to head injury, shock, intoxication); and edema or hematoma due to direct neck trauma. These obstructions are readily visible on direct inspection of the mouth or neck; having the patient speak can rapidly confirm that the airway is not likely in immediate danger.
Blood and foreign material are removed by suction or manually. Obtunded patients whose airway patency, airway protective mechanisms, oxygenation, or ventilation is in doubt and patients with significant oropharyngeal injury require endotracheal intubation; usually drugs are given to induce unconsciousness and paralysis before intubation is done. Multiple tools are available to assist with airway management including extraglottic devices, airway bougie, and video laryngoscopy. A carbon dioxide colorimetric device or, preferably, waveform capnography can help confirm proper endotracheal tube placement.
If patients require an artificial airway and endotracheal intubation is not possible (eg, due to edema of the airway caused by a thermal burn) or contraindicated (eg, due to severe maxillofacial injury), surgical or percutaneous cricothyrotomy is indicated. NOTE: When evaluating or manipulating a patient’s airway, cervical spine immobilization should be maintained (eg, by rigid collar, inline immobilization techniques) until cervical spine injury has been excluded by examination, imaging, or both.
Breathing
Adequate ventilation is threatened by decreased central respiratory drive (usually due to head injury, intoxication, or nearly fatal shock) or by chest injury (eg, hemothorax or pneumothorax, multiple rib fractures, pulmonary contusion).
The chest wall is fully exposed to look for ample chest wall expansion, external signs of trauma, and paradoxical wall motion (ie, retraction of the chest wall on inspiration), which indicates a flail chest. The chest wall is palpated for rib fractures and the presence of subcutaneous air (sometimes the only finding in pneumothorax).
Adequacy of air exchange is usually apparent on auscultation. Tension pneumothorax, simple pneumothorax, or hemothorax may cause decreased breath sounds on the affected side. Tension pneumothorax may also cause distended neck veins; hypotension and deviation of the trachea to the side opposite the injury are later findings.
Pneumothorax is decompressed by chest tube (see How To Do Tube Thoracostomy). In patients with findings consistent with a pneumothorax, a chest x-ray or bedside ultrasonography should be done before initiating positive-pressure ventilation. Positive-pressure ventilation may enlarge a simple pneumothorax or convert it to a tension pneumothorax. Suspected tension pneumothorax can be decompressed with finger thoracostomy (insertion of a finger into the pleural space) or needle thoracostomy (eg, a 14-gauge needle inserted in the midaxillary line, 5th intercostal space) to stabilize the patient if a chest tube cannot be inserted immediately. Inadequate ventilation is treated with endotracheal intubation and mechanical ventilation. An open pneumothorax is covered with an occlusive dressing attached on 3 sides; the 4th side is left untaped to release pressure that might build up and cause a tension pneumothorax.
Circulation
Significant external hemorrhage can occur from any major vessel but is always apparent. Life-threatening internal hemorrhage is often less obvious. However, this volume of hemorrhage can occur in only a few body compartments: the chest, abdomen, retroperitoneum, and soft tissues of the pelvis or thigh (eg, from a pelvic or femoral fracture).
Pulse and blood pressure are assessed, and signs of shock are noted (eg, tachypnea, dusky color, diaphoresis, altered mental status, poor capillary refill). Abdominal distention and tenderness, pelvis instability, and thigh deformity and instability are often present when internal hemorrhage in those areas is large enough to be life threatening.
External hemorrhage is controlled by direct pressure. Tourniquets should be applied for extremity bleeding if bleeding is not controlled by direct pressure. Two large-bore (eg, 14- or 16-gauge) IVs are started with 0.9% saline or lactated Ringer's solution; rapid infusion of 1 L (20 mL/kg for children) is given for signs of shock and hypovolemia
When there is strong clinical suspicion of serious intra-abdominal hemorrhage, patients may require immediate laparotomy. Placement of a resuscitative balloon for occlusion of the aorta can help stabilize the patient before surgery. Patients with massive intrathoracic hemorrhage may require immediate thoracotomy and possibly autotransfusion of blood recovered via tube thoracostomy.
Pearls & Pitfalls
|
Disability (neurologic dysfunction)
Neurologic function is evaluated for serious deficits involving the brain and spinal cord. The Glasgow Coma Scale (GCS; see tables Glasgow Coma Scale and Modified Glasgow Coma Scale for Infants and Children) and pupillary response to light are used to assess the level of consciousness and severity of intracranial injury.
Gross motor movement and sensation in each extremity are used to screen for serious spinal cord injury. The cervical spine is palpated for tenderness and deformity and stabilized in a rigid collar until cervical spine injury is excluded. With careful manual stabilization of the head and neck, the patient is logrolled onto a side to allow
Palpation of the thoracic and lumbar spine
Inspection of the back
Rectal examination if indicated to check tone (decreased tone indicates possible spinal cord injury), the prostate (a high-riding prostate suggests urethral or pelvic injury), and presence of blood
In the US, most patients arriving by ambulance are immobilized on a long, rigid board for ease of transport and to stabilize possible spinal fractures. Patients should be taken off the board as soon as possible because it is quite uncomfortable and pressure ulcers may occur within a few hours.
Patients with severe traumatic brain injury (GCS < 8) may require endotracheal intubation for airway protection, brain imaging, neurosurgical evaluation, and therapy to prevent secondary brain injury (eg, optimization of blood pressure and oxygenation, seizure prophylaxis, treatment of elevated intracranial pressure, sometimes transient hyperventilation for patients with signs of impending brain herniation).
Exposure/environmental control
To ensure injuries are not missed, patients are completely undressed (by cutting off garments) and the entire body surface is examined for signs of occult trauma. The patient is kept warm (eg, with heated blankets and by using warmed IV fluids) to prevent hypothermia.
Secondary survey
After immediate life threats are assessed and the patient is stable, a more thorough evaluation is done, and a focused history is obtained. If only limited conversation is possible, an “AMPLE” history covers essential information:
Allergies
Medications
Past medical history
Last meal
Events of the injury
After the patient is completely undressed, the examination generally proceeds from head to toe; it typically includes all orifices and a more detailed look at areas examined in the initial survey. All soft tissues are inspected for lesions and swelling, all bones are palpated for tenderness, and range of motion is assessed in joints (unless there is obvious fracture or deformity).
A urinary catheter is usually placed in seriously injured and obtunded patients provided there is no evidence of urethral injury (eg, blood at the meatus, ecchymosis of the perineum). Intubated, seriously injured patients often also have an orogastric tube placed.
Open wounds are covered with sterile dressings, but cleansing and repair are deferred until completion of evaluation and treatment of more serious injuries. Serious clinically apparent dislocations with marked deformity or neurovascular compromise are imaged and reduced as soon as immediate life threats have been addressed.
Obvious or suspected fractures are splinted pending full assessment of serious injuries and appropriate imaging studies. A clinically apparent unstable pelvic fracture is stabilized with a commercial pelvic binder or bed sheet to help close the pelvic space and decrease bleeding; severe bleeding may require urgent angiographic embolization, surgical fixation, or direct surgical control.
In pregnant trauma patients, the initial priority is stabilization of the woman, which is the best way to ensure fetal stability. Near term, immobilization in the supine position may cause the uterofetoplacental unit to compress the inferior vena cava, obstructing blood return and causing hypotension. If so, the uterus can be manually pushed to the patient's left or the entire backboard can be tilted to the left to relieve the compression. Fetal monitoring is done if the fetus is >20 weeks gestation and continued for at least 4 to 6 hours. An obstetrician should be consulted early for patients with serious trauma or signs of pregnancy complications (eg, abnormal fetal heart rate, vaginal bleeding, contractions). Rh0(D) immune globulin is given to all Rh-negative women following even minor trauma. If the woman has cardiac arrest and cannot be resuscitated, a perimortem cesarean delivery can be done if the fetus is >20 weeks' gestation (corresponding to a uterine fundal height above the umbilicus).
Testing
Imaging and laboratory tests supplement clinical assessment. Patients with penetrating trauma typically have focal injuries that can limit imaging to the obviously involved region or regions. Blunt trauma, particularly when significant deceleration is involved (eg, serious fall, motor vehicle crash), can affect any part of the body, and imaging is used more liberally. Previously, x-rays or CT of the neck, chest, and pelvis were routinely done on most patients with blunt trauma. However, most trauma centers are now doing only imaging studies that are indicated by the mechanism of injury and findings on examination.
Cervical spine imaging can be deferred in patients who are not intoxicated, do not have focal neurologic findings, have no midline cervical spine tenderness or distracting injuries (eg, femur fracture), and are awake and alert. All others should have cervical spine imaging, preferably using CT.
Chest x-ray can identify airway disruption, lung injury, hemothorax, and pneumothorax; it can also suggest thoracic aorta tears (eg, by mediastinal widening). However, chest CT is more sensitive for most intrathoracic injuries and is often preferred. Chest imaging is now commonly done at the bedside using ultrasonography E-FAST (extended focused assessment with sonography in trauma), particularly if patients are unstable. Pneumothoraces, hemothoraces, and hemopericardium can be identified.
CT of the chest, abdomen, pelvis, spine, or head or, particularly, combinations of these studies are frequently used for patients who require imaging after severe multiple blunt trauma.
Identification of intra-abdominal injury is essential. Historically, diagnostic peritoneal lavage (DPL) was used to assess for intraperitoneal blood. In DPL, a peritoneal dialysis catheter is inserted through the abdominal wall into the peritoneal cavity. If >10 mL of blood is aspirated, immediate laparotomy is indicated. If blood is not aspirated, 1 L of 0.9% saline is infused through the catheter and drained out; analysis of the returned fluid is used to guide management. However, in all but low-resource areas, DPL has largely been replaced by bedside ultrasonography (E-FAST examination), particularly for unstable patients; it is sensitive for significant volumes of intraperitoneal blood and thus the need for immediate laparotomy. If patients are stable, CT is the preferred study; it is very accurate, allows imaging of the retroperitoneal structures and bones, and shows the volume and sometimes the origin of hemorrhage.
If pelvic fracture is suspected, CT of the pelvis is done; it is more accurate than plain x-rays.
Head CT is typically done in patients with altered mental status or focal neurologic abnormalities and in patients who sustained loss of consciousness. Some evidence suggests that CT is not necessary in patients with brief loss of consciousness (ie, < 5 seconds) or transient amnesia or disorientation but who are alert with a GCS of 15 during examination. Imaging is done more liberally in patients with persistent headache, vomiting, amnesia, seizures, age > 60 years, and drug or alcohol intoxication and in patients taking anticoagulant or antiplatelet drugs. Clinical decision rules have been developed to help determine which patients should have a head CT (1). These decision rules should be used to aid, but not replace, clinical judgment.
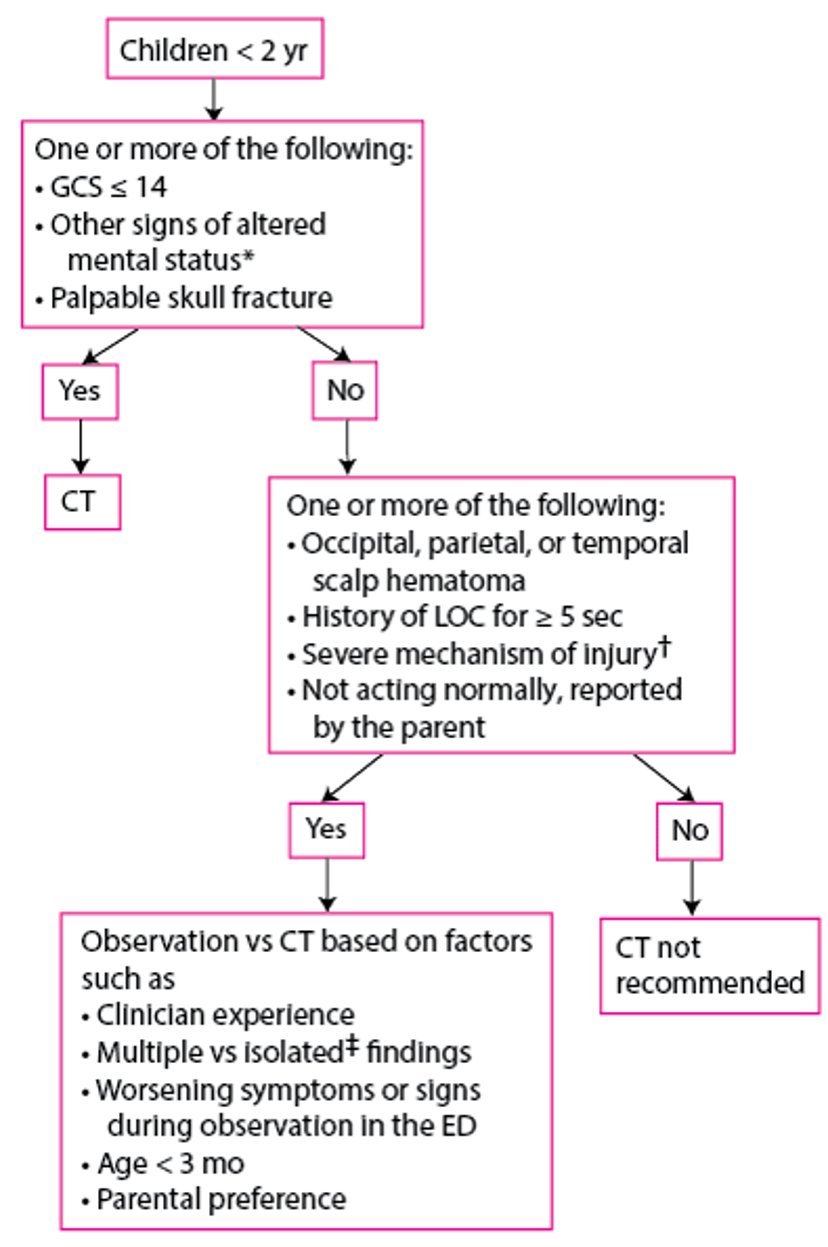
For children with head injury, the Pediatric Emergency Care Applied Research Network (PECARN) has developed an algorithm that may help limit radiation exposure from head CT; clinical observation is used in children who may otherwise have received CT.
Evaluation of Children 0 to 2 Years With a Head Injury
* Include agitation, somnolence, repetitive questioning, and slow response to verbal communication. |
† Include motor vehicle crash involving ejection of patient, death of another passenger, or rollover; collision of a motor vehicle with a pedestrian or bicyclist not wearing a helmet; and a fall of > 0.9 m for children < 2 years; and a blow to the head by a high-impact object. |
‡ No other findings suggesting traumatic brain injury, such as only LOC, headache, vomiting, and certain scalp hematomas in children >3 months. |
ED = emergency department; GCS = Glasgow Coma Scale; LOC = loss of consciousness. |
Adapted from Kupperman N, Holmes JF, Dayan PS, et al for the Pediatric Emergency Care Applied Research Network: Identification of children at very low risk of clinically-important brain injuries after head trauma: A prospective cohort study. Lancet 374: 1160-1170, 2009. doi:10.1016/S0140-6736(09)61558-0 |

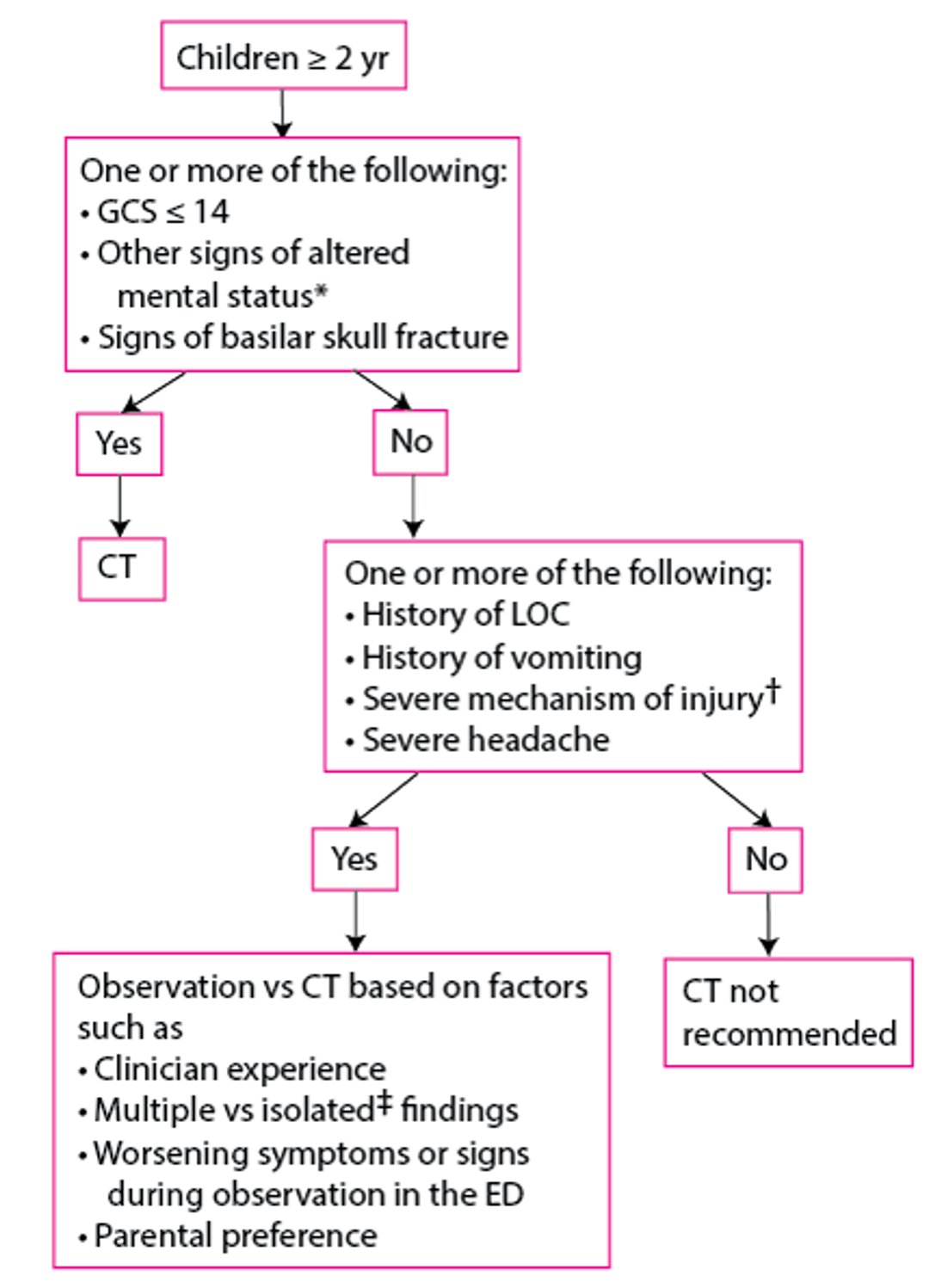
Evaluation of Children ≥ 2 Years With a Head Injury
* Include agitation, somnolence, repetitive questioning, and slow response to verbal communication. |
† Include motor vehicle crash involving ejection of patient, death of another passenger, or rollover; collision of a motor vehicle with a pedestrian or bicyclist not wearing a helmet; and a fall of >1.5 m for children ≥ 2 years; and a blow to the head by a high-impact object. |
‡ No other findings suggesting traumatic brain injury, such as only LOC, headache, vomiting, and certain scalp hematomas in children >3 months. |
ED = emergency department; GCS = Glasgow Coma Scale; LOC = loss of consciousness. |
Adapted from Kupperman N, Holmes JF, Dayan PS, et al for the Pediatric Emergency Care Applied Research Network: Identification of children at very low risk of clinically-important brain injuries after head trauma: A prospective cohort study. Lancet 374: 1160-1170, 2009. doi:10.1016/S0140-6736(09)61558-0 |

Patients with suspected spinal cord injury should be imaged using MRI.
Aortic injury should be considered in patients with severe deceleration chest injury or suggestive signs (eg, pulse deficits or asymmetric blood pressure measurements, end-organ ischemia, suggestive findings on chest x-ray); these patients may require CT angiography or other aortic imaging (see Aortic Disruption [Traumatic]). Short-acting beta blockers can be used to control heart rate and blood pressure in patients with traumatic aortic injury.
All patients suspected of having significant blunt chest injury should be placed on a cardiac monitor and have an ECG to detect myocardial injury and arrhythmias. Patients with abnormalities on ECG usually have blood levels of cardiac markers measured and sometimes echocardiography to evaluate the patient for possible cardiac contusion.
Vascular injury to the carotid and vertebral vessels should be considered in patients with trauma to the head and neck, particularly those with unilateral neurologic findings, a neck seat belt sign (linear ecchymosis due to the shoulder strap), or a predisposing injury (eg, fracture of C1, C2, or C3; other C-spine fracture with subluxation; hanging mechanism). Such patients typically should have CT angiography.
Plain x-rays are obtained of any suspected fractures and dislocations of the extremities. Other imaging tests are obtained for specific indications (eg, angiography to diagnose and sometimes embolize vascular injury; CT to better delineate spinal, pelvic, or complex joint fractures).
Laboratory tests that may be useful include
Complete blood count to establish a baseline
Serial hemoglobin levels to assess for bleeding
Blood gas determination for partial pressure of oxygen, partial pressure of carbon dioxide, and base deficit
Urine examination for blood
Glucose to evaluate for hypoglycemia
Type and crossmatch for possible blood transfusion
Coagulation studies
Measures of perfusion (serum lactate, base deficit on arterial blood gas measurement, and, in patients with a catheterized central vein, central venous oxygen saturation) are indicated to help identify early or partially treated shock. Other reflexively obtained tests (eg, electrolytes and other chemistries) are unlikely to be helpful unless suggested by relevant medical history (eg, renal insufficiency, diuretic use).
Toxicology screening (eg, blood alcohol, urine drug screen) is often done; results of this testing rarely change immediate management but can help identify substance use disorder causative of injury, allowing intervention to prevent subsequent trauma.
D-Dimer, fibrinogen, and fibrin degradation products may be measured in pregnant trauma patients. Test results may be abnormal in patients with placental abruption; however, these tests are neither sensitive nor specific and cannot definitively confirm or exclude the diagnosis.
Evaluation and treatment reference
1. Bouida W, Marghli S, Souissi S, et al: Prediction value of the Canadian CT head rule and the New Orleans criteria for positive head CT scan and acute neurosurgical procedures in minor head trauma: A multicenter external validation study. Ann Emerg Med 61(5): 521-527, 2013. doi: 10.1016/j.annemergmed.2012.07.016
More Information
The following English-language resources may be useful. Please note that THE MANUAL is not responsible for the content of these resources.
American College of Surgeons Revised Statement on Trauma Center Designation Based Upon System Need and the Economic Drivers Impacting Trauma Systems: This addendum to the 2014 statement was added in June 2021 to address specific issues related to the economic drivers that have an impact on trauma systems.
Pediatric Emergency Care Applied Research Network (PECARN): This site provides information about multi-center research on the prevention and management of acute illnesses and injuries in children.




