

Heart failure (HF) is a clinical syndrome in which the heart is not able to meet the metabolic demands of the body due to a structural and or functional cardiac abnormality, leading to low cardiac output, elevated ventricular filling pressure, or both. HF can involve systolic and/or diastolic function, in the left and/or right heart. Left ventricular (LV) failure typically causes shortness of breath and fatigue, and right ventricular (RV) failure typically causes peripheral and abdominal fluid accumulation; the ventricles can be involved together or separately. Diagnosis is initially clinical, supported by chest radiography, echocardiography, hemodynamic evaluation, and laboratory testing. Treatment includes patient education, treating the cause(s) of the HF syndrome, pharmacologic therapy including neurohormonal modulation, implantable pacemakers/defibrillators, mechanical circulatory support, and heart transplantation.
Heart failure affects more than 64 million people worldwide (1). In the United States, there are approximately 6.7 million people with heart failure and approximately 1 million new cases per year; 8.7 million people are projected to have heart failure by 2030 (2, 3).
(See also table .)
General references
1. Savarese G, Becher PM, Lund LH, Seferovic P, Rosano GMC, Coats AJS. Global burden of heart failure: a comprehensive and updated review of epidemiology [published correction appears in Cardiovasc Res. 2023 Jun 13;119(6):1453. doi: 10.1093/cvr/cvad026.]. Cardiovasc Res. 2023;118(17):3272-3287. doi:10.1093/cvr/cvac013
2. Bozkurt B, Ahmad T, Alexander K, et al. HF STATS 2024: Heart Failure Epidemiology and Outcomes Statistics An Updated 2024 Report from the Heart Failure Society of America. J Card Fail. 2025;31(1):66-116. doi:10.1016/j.cardfail.2024.07.001
3. Virani SS, Alonso A, Benjamin EJ, et al. Heart Disease and Stroke Statistics-2020 Update: A Report From the American Heart Association. Circulation. 2020;141(9):e139-e596. doi:10.1161/CIR.0000000000000757
Cardiovascular Physiology
Cardiac contractility (force and velocity of contraction), ventricular performance, and myocardial oxygen requirements are determined by:
Preload
Afterload
Substrate availability (eg, oxygen, fatty acids, glucose)
Heart rate and rhythm
Amount of viable myocardium
Cardiac output is the product of stroke volume and heart rate; it is also affected by venous return, peripheral vascular tone, and neurohumoral factors.
Preload is the loading condition of the heart at the end of its relaxation and filling phase (diastole) just before contraction (systole). Preload represents the degree of end-diastolic fiber stretch and end-diastolic volume, which is influenced by ventricular diastolic volume and pressure and the composition of the myocardial wall. Typically, left ventricular (LV) end-diastolic pressure, especially if higher than normal, is a reasonable measure of preload. LV dilation, hypertrophy, and changes in myocardial distensibility (compliance) modify preload. Preload is not identical to, but is largely a function of, the body's overall intravascular volume status.
Afterload is the force resisting myocardial fiber contraction at the start of systole. It is determined by LV chamber pressure, radius, and wall thickness at the time the aortic valve opens. Clinically, systemic systolic blood pressure at or shortly after the aortic valve opens correlates with peak systolic wall stress and approximates afterload.
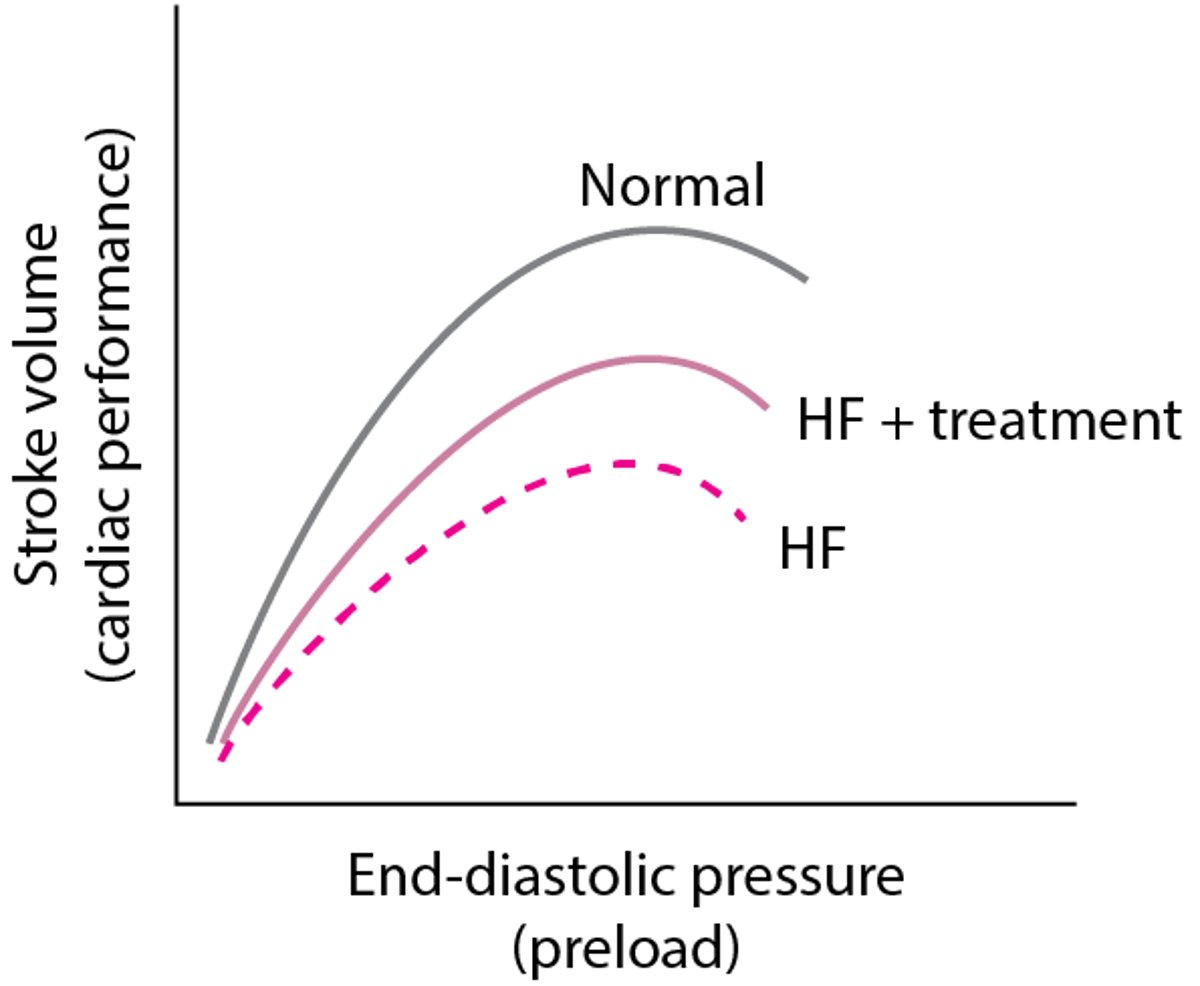
The Frank-Starling principle describes the relationship between preload and cardiac performance. It states that, normally, systolic performance (often estimated by stroke volume) is proportional to preload within the normal physiologic range (see figure ). In patients with heart failure, systolic performance and myocardial contractility are reduced when compared to those with a healthy heart at the same preload. Contractility is difficult to measure clinically (because it requires cardiac catheterization with pressure-volume analysis) but is reasonably reflected by the ejection fraction (EF), which is the percentage of end-diastolic volume ejected with each contraction (stroke volume/end-diastolic volume). EF can generally be adequately assessed noninvasively with echocardiography, nuclear imaging, or MRI.
The force-frequency relationship refers to the phenomenon in which repetitive stimulation of a muscle within a certain frequency range results in increased force of contraction. Normal cardiac muscle at typical heart rates exhibits a positive force-frequency relationship, so a faster rate causes stronger contraction (and corresponding greater substrate requirements). During some types of heart failure, the force-frequency relationship may become negative, so that myocardial contractility decreases as heart rate increases above a certain rate.
Cardiac reserve is the ability of the heart to increase its performance above resting levels in response to emotional or physical stress; body oxygen consumption may increase from 250 mL/minute to ≥ 1500 mL/minute during maximal exertion. Mechanisms include:
Increasing heart rate
Increasing diastolic filling volumes
Increasing contractility and stroke volume
Selectively altering systemic vascular resistance to direct blood flow toward certain organs (eg, skeletal muscle during exercise)
Increasing tissue extraction of oxygen (the difference between oxygen content in arterial blood and in mixed venous or pulmonary artery blood)
In well-trained young adults during maximal exercise, heart rate may increase from 55 to 70 beats/minute at rest to > 180 beats/minute, and cardiac output may increase from 6 L/minute to ≥ 25 L/minute. At rest, arterial blood contains approximately 18 mL oxygen/dL of blood, and mixed venous or pulmonary artery blood contains approximately 14 mL/dL. Oxygen extraction is thus approximately 4 mL/dL. When demand is increased, oxygen extraction may increase to 12 to 14 mL/dL. This mechanism also helps compensate for reduced tissue blood flow in heart failure.
Frank-Starling Principle
Normally (top curve), as preload increases, cardiac performance also increases. However, at a certain point, performance plateaus, then declines. In heart failure (HF) due to systolic dysfunction (bottom curve), the overall curve shifts downward, reflecting reduced cardiac performance at a given preload, and as preload increases, cardiac performance increases less. With treatment (middle curve), performance is improved, although not normalized. |

Pathophysiology of Heart Failure
In heart failure, the heart may not provide tissues with adequate blood for metabolic needs, and cardiac-related elevation of pulmonary or systemic venous pressures may result in organ congestion. This condition can result from abnormalities of systolic or diastolic function or, commonly, both. Although a primary abnormality can be a change in cardiomyocyte function, there are also changes in collagen turnover of the extracellular matrix. Cardiac structural defects (eg, congenital defects, valvular disorders), rhythm abnormalities (including persistently high heart rate), and high metabolic demand (eg, due to thyrotoxicosis) also can cause heart failure.

Classification of heart failure
Heart failure can be classified as primarily left or right heart failure, or by the Universal Definition and Classification of Heart Failure (1), which uses the left ventricular ejection fraction.
The traditional distinction between left and right ventricular failure is somewhat misleading because the heart is an integrated pump, and changes in one chamber ultimately affect the whole heart. However, these terms indicate the major site of pathology leading to heart failure and can be useful for initial evaluation and treatment. Other common terms used to differentiate types of and causes for heart failure include acute or chronic; high output or low output; dilated or nondilated; and ischemic, hypertensive, or idiopathic dilated cardiomyopathy. Treatment also differs based on whether the presentation is acute or chronic HF.
LV failure
Heart failure most commonly occurs as a result of left ventricular dysfunction (2). As a result, the Universal Classification of Heart Failure has categorized heart failure according to reduced, preserved, minimally reduced, and improved ejection fraction based on left ventricular systolic function (1). In left heart failure, cardiac output decreases and pulmonary venous pressure increases. When pulmonary capillary pressure exceeds the oncotic pressure of plasma proteins (approximately 24 mm Hg), fluid extravasates from the capillaries into the interstitial space and alveoli, reducing pulmonary compliance and increasing the work of breathing. Lymphatic drainage increases but cannot compensate for the increase in pulmonary fluid. Marked fluid accumulation in alveoli (pulmonary edema) significantly alters ventilation-perfusion (V/Q) relationships. Deoxygenated pulmonary arterial blood passes through poorly ventilated alveoli, decreasing systemic arterial oxygenation (partial pressure of arterial oxygen [PaO2]) and causing dyspnea. However, dyspnea may occur before V/Q abnormalities, probably because of elevated pulmonary venous pressure and increased work of breathing; the precise mechanism is unclear.
In severe or chronic LV failure, pleural effusions characteristically develop, further aggravating dyspnea. Minute ventilation increases; thus, partial pressure of arterial carbon dioxide (PaCO2) decreases and blood pH increases (respiratory alkalosis). Marked interstitial edema of the small airways may interfere with ventilation, elevating PaCO2—a sign of impending respiratory failure.
Heart failure with reduced ejection fraction (HFrEF)
In HFrEF (also called systolic heart failure), global LV systolic dysfunction predominates. The LV contracts poorly and empties inadequately, leading to:
Increased diastolic volume and pressure
Decreased ejection fraction (≤ 40%)
Many defects in energy utilization, energy supply, electrophysiologic function, and contractile element interaction occur, with abnormalities in intracellular calcium modulation and cyclic adenosine monophosphate (cAMP) production.
Predominant systolic dysfunction is common in heart failure due to myocardial infarction, myocarditis, and dilated cardiomyopathy. Systolic dysfunction may affect primarily the LV or the right ventricle (RV); LV failure often leads to RV failure.
Heart failure with preserved ejection fraction (HFpEF)
In HFpEF (also called diastolic heart failure), LV filling is impaired, resulting in:
Increased LV end-diastolic pressure at rest or during exertion
Usually, normal LV end-diastolic volume
Global contractility and hence LV ejection fraction remain normal (≥ 50%).
However, in some patients, marked restriction to LV filling can cause inappropriately low LV end-diastolic volume and thus cause low cardiac output and systemic symptoms. Elevated left atrial pressures can cause pulmonary hypertension and pulmonary congestion.
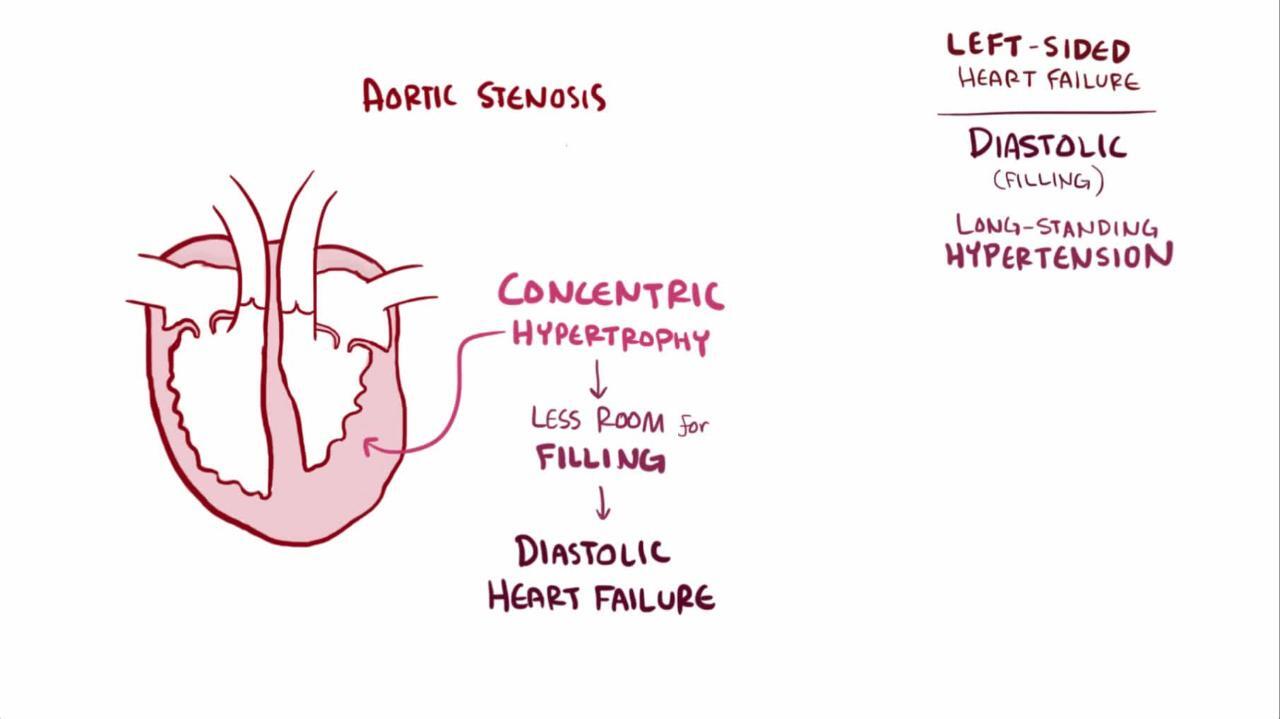
Diastolic dysfunction usually results from impaired ventricular relaxation (an active process), increased ventricular stiffness, valvular disease, or constrictive pericarditis. Acute myocardial ischemia is also a cause of diastolic dysfunction. Resistance to filling increases with age, reflecting cardiomyocyte dysfunction and cardiomyocyte loss, and increased interstitial collagen deposition; thus, diastolic dysfunction is particularly common among older adults. Diastolic dysfunction predominates in hypertrophic cardiomyopathy, other disorders with ventricular hypertrophy (eg, hypertension, significant aortic stenosis), and amyloid infiltration of the myocardium. LV filling and function may also be impaired if marked increases in RV pressure shift the interventricular septum to the left.
Diastolic dysfunction is recognized as an important cause of HF. Approximately 50% of patients with heart failure have HFpEF; the prevalence increases with age and in patients with diabetes (3). HFpEF is a complex, heterogenous, multiorgan, systemic syndrome, often with multiple concomitant pathophysiologies. Data suggest that multiple comorbidities (eg, obesity, hypertension, diabetes, chronic kidney disease) lead to systemic inflammation, widespread endothelial dysfunction, cardiac microvascular dysfunction, and, ultimately, molecular changes in the heart that cause increased myocardial fibrosis and ventricular stiffening. Thus, although HFrEF is typically associated with primary myocardial injury, HFpEF may be associated with secondary myocardial injury due to abnormalities in the periphery.
Heart failure with mildly reduced ejection fraction (HFmrEF)
HF with mildly reduced ejection fraction (HFmrEF) is defined as an LV ejection fraction of 41 to 49%. It is unclear whether this group is a distinct population or consists of a mixture of patients with either HFpEF or HFrEF.
Heart failure with improved ejection fraction (HFimpEF)
Patients with HF whose LV ejection fraction has improved by more than an absolute of 10% from a prior value and also measures over 40% are categorized as having HFimpEF.
RV failure
Right ventricular failure most commonly occurs as a consequence of or in tandem with left ventricular failure. Isolated right heart failure is observed much less commonly. In heart failure that involves right ventricular dysfunction (see Right Heart Failure), systemic venous pressure increases, causing fluid extravasation and consequent edema, primarily in dependent tissues (feet and ankles of ambulatory patients) and abdominal viscera. The liver is most severely affected, but the stomach and intestine also become congested; fluid accumulation in the peritoneal cavity (ascites) can occur. RV failure commonly causes moderate hepatic dysfunction, with usually modest increases in conjugated and unconjugated bilirubin, prothrombin time (PT), and hepatic enzymes (particularly alkaline phosphatase and gamma-glutamyl transpeptidase [GGT]). The impaired liver breaks down less aldosterone, further contributing to fluid accumulation. Chronic venous congestion in the viscera can cause anorexia, malabsorption of nutrients and medications, protein-losing enteropathy (characterized by diarrhea and marked hypoalbuminemia), chronic gastrointestinal blood loss, and rarely ischemic bowel infarction.
Responses to heart failure
Myocardial response
When left ventricular contractility is impaired, as is the case in HFrEF, a higher preload is required to maintain cardiac output. As a result, the ventricles are remodeled over time. During remodelling, the LV becomes less ovoid and more spherical, dilates, and hypertrophies; the RV dilates and may hypertrophy. Initially compensatory, remodelling ultimately is associated with adverse outcomes because the changes eventually increase diastolic stiffness and wall tension (ie, diastolic dysfunction develops), compromising cardiac performance, especially during physical stress. Increased wall stress raises oxygen demand and accelerates apoptosis (programmed cell death) of myocardial cells. Dilation of the ventricles can also cause mitral or tricuspid valve regurgitation (due to annular dilation) with further increases in end-diastolic volumes.
Hemodynamic response
With reduced cardiac output, oxygen delivery to the tissues is maintained by increasing oxygen extraction from the blood and sometimes shifting the oxyhemoglobin dissociation curve (see figure ) to the right to favor oxygen release.
Reduced cardiac output with lower systemic blood pressure activates arterial baroreflexes, increasing sympathetic tone and decreasing parasympathetic tone. As a result, heart rate and myocardial contractility increase, arterioles in selected vascular beds constrict, venoconstriction occurs, and sodium and water are retained. These changes compensate for reduced ventricular performance and help maintain hemodynamic homeostasis in the early stages of heart failure. However, these compensatory changes increase cardiac work, preload, and afterload; reduce coronary and renal perfusion; cause fluid accumulation resulting in congestion; increase potassium excretion; and may cause cardiomyocyte necrosis and arrhythmias.
Renal response
As cardiac function deteriorates, renal blood flow decreases due to low cardiac output. In addition, renal venous pressures increase, leading to renal venous congestion. These changes result in a decrease in glomerular filtration rate (GFR), and blood flow within the kidneys is redistributed. The filtration fraction and filtered sodium decrease, but tubular resorption increases, leading to sodium and water retention. Blood flow is further redistributed away from the kidneys during exercise, but renal blood flow improves during rest.
Decreased perfusion of the kidneys (and possibly decreased arterial systolic stretch secondary to declining ventricular function) activates the renin-angiotensin-aldosterone system, increasing sodium and water retention and renal and peripheral vascular tone. These effects are amplified by the intense sympathetic activation accompanying heart failure.
The renin-angiotensin-aldosterone-vasopressin (antidiuretic hormone [ADH]) system causes a cascade of potentially deleterious long-term effects. Angiotensin II worsens heart failure by causing vasoconstriction, including efferent renal vasoconstriction, and by increasing aldosterone production, which enhances sodium reabsorption in the distal nephron and also causes myocardial and vascular collagen deposition and fibrosis. Angiotensin II increases norepinephrine release, stimulates release of vasopressin, and triggers apoptosis. Angiotensin II may be involved in vascular and myocardial hypertrophy, thus contributing to the remodeling of the heart and peripheral vasculature, potentially worsening heart failure. Aldosterone can be synthesized in the heart and vasculature independently of angiotensin II (perhaps mediated by corticotropin, nitric oxide, free radicals, and other stimuli) and may have deleterious effects in these organs.
Heart failure that causes progressive renal dysfunction (including renal dysfunction caused by medications used to treat HF) contributes to worsening HF and has been termed the cardiorenal syndrome.
Neurohumoral response
In conditions of stress, neurohumoral responses help increase heart function and maintain blood pressure and organ perfusion. Chronic activation of these responses is detrimental to the normal balance between myocardial-stimulating and vasoconstricting hormones and between myocardial-relaxing and vasodilating hormones.
The heart contains many neurohumoral receptors (alpha-1, beta-1, beta-2, beta-3, angiotensin II type 1 [AT1] and type 2 [AT2], muscarinic, endothelin, serotonin, adenosine, cytokine, natriuretic peptides); the roles of all of these receptors are not fully defined. In patients with heart failure, beta-1 receptors (which constitute 70% of cardiac beta receptors) are downregulated, probably in response to intense sympathetic activation. The result of downregulation is impaired myocyte contractility and increased heart rate.
Plasma norepinephrine levels are increased, largely reflecting sympathetic nerve stimulation as plasma epinephrine levels are not increased. Detrimental effects include vasoconstriction with increased preload and afterload, direct myocardial damage including apoptosis, reduced renal blood flow, and activation of other neurohumoral systems, including the renin-angiotensin-aldosterone-vasopressin system.
Vasopressin is released in response to a fall in blood pressure via various neurohormonal stimuli. Increased vasopressin decreases renal excretion of free water, possibly contributing to hyponatremia in heart failure. Vasopressin levels in patients with HF and normal blood pressure vary.
Atrial natriuretic peptide is released in response to increased atrial volume and pressure; brain (B-type) natriuretic peptide (BNP) is released from the ventricle in response to ventricular stretching. These peptides enhance renal excretion of sodium; however, in patients with HF, the effect is blunted by decreased renal perfusion pressure, receptor downregulation, and perhaps enhanced enzymatic degradation. In addition, elevated levels of natriuretic peptides exert a counter-regulatory effect on the renin-angiotensin-aldosterone system and catecholamine stimulation.
Because endothelial dysfunction occurs in HF, fewer endogenous vasodilators (eg, nitric oxide, prostaglandins) are produced, and more endogenous vasoconstrictors (eg, endothelin) are produced, thus increasing afterload.
The failing heart and other organs produce tumor necrosis factor (TNF) alpha. This cytokine increases catabolism and is possibly responsible for cardiac cachexia (loss of lean tissue ≥ 10%), which may accompany severely symptomatic HF, and for other detrimental changes. The failing heart also undergoes metabolic changes with increased free fatty acid utilization and decreased glucose utilization; these changes may become therapeutic targets.
Changes with aging
Age-related changes in the heart and cardiovascular system lower the threshold for expression of heart failure. Interstitial collagen within the myocardium increases, the myocardium stiffens, and myocardial relaxation is prolonged. These changes lead to a significant reduction in diastolic left ventricular function, even in healthy older adults. Modest decline in systolic function also occurs with aging. An age-related decrease in myocardial and vascular responsiveness to beta-adrenergic stimulation further impairs the ability of the cardiovascular system to respond to increased work demands.
As a result of these changes, peak exercise capacity decreases significantly (approximately 8%/decade after age 30 years), and cardiac output at peak exercise decreases more modestly. This decline can be slowed by regular physical exercise. Thus, older patients are more prone than are younger ones to develop HF symptoms in response to the stress of systemic disorders or relatively modest cardiovascular insults. Stressors include infections (particularly pneumonia), hyperthyroidism, anemia, hypertension, myocardial ischemia, hypoxia, hyperthermia, renal failure, perioperative IV fluid loads, nonadherence to medication regimens or to low-salt diets, and use of certain medications (particularly nonsteroidal anti-inflammatory drugs [NSAIDs]).
Pathophysiology references
1. Bozkurt B, Coats AJ, Tsutsui H, et al. Universal Definition and Classification of Heart Failure: A Report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure. J Card Fail. Published online March 1, 2021. doi:10.1016/j.cardfail.2021.01.022
2. Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines [published correction appears in J Am Coll Cardiol. 2023 Apr 18;81(15):1551. doi: 10.1016/j.jacc.2023.03.002.]. J Am Coll Cardiol. 2022;79(17):e263-e421. doi:10.1016/j.jacc.2021.12.012
3. Campbell P, Rutten FH, Lee MM, Hawkins NM, Petrie MC. Heart failure with preserved ejection fraction: everything the clinician needs to know [published correction appears in Lancet. 2024 Mar 16;403(10431):1026. doi: 10.1016/S0140-6736(24)00494-X.]. Lancet. 2024;403(10431):1083-1092. doi:10.1016/S0140-6736(23)02756-3
Etiology of Heart Failure
Both cardiac and systemic factors can impair cardiac performance and cause or aggravate heart failure (see table ).
Causes of Heart Failure
Type | Examples |
|---|---|
Cardiac | |
Myocardial damage | Some chemotherapy agents |
Valvular disorders | |
Arrhythmias | Bradyarrhythmias Tachyarrhythmias |
Conduction defects | |
Reduced substrate availability (eg, of free fatty acids or glucose) | Ischemia |
Infiltrative or matrix disorders | Chronic fibrosis (eg, systemic sclerosis) |
Systemic | |
Disorders that increase demand for cardiac output | |
Disorders that increase resistance to output (afterload) | |
LV failure characteristically develops in ischemic heart disease, hypertension, mitral regurgitation, aortic regurgitation, aortic stenosis, most forms of cardiomyopathy, and congenital heart disorders (eg, ventricular septal defect, patent ductus arteriosus with large shunts).
RV failure is most commonly caused by previous LV failure (which increases pulmonary venous pressure and leads to pulmonary hypertension, thus overloading the RV) or by a severe lung disorder (in which case it is called cor pulmonale). Other causes are multiple pulmonary emboli, RV infarction, pulmonary arterial hypertension, tricuspid regurgitation, tricuspid stenosis, mitral stenosis, pulmonary artery stenosis, pulmonic valve stenosis, pulmonary venous occlusive disease, arrhythmogenic right ventricular cardiomyopathy, or congenital disorders such as Ebstein anomaly or Eisenmenger syndrome. Some conditions mimic RV failure, except cardiac function may be normal; they include volume overload and increased systemic venous pressure in polycythemia or overtransfusion, acute kidney injury with retention of sodium and water, obstruction of either vena cava, and hypoproteinemia due to any cause resulting in low plasma oncotic pressure and peripheral edema.
Biventricular failure results from disorders that affect the whole myocardium (eg, viral myocarditis, amyloidosis, Chagas disease) or long-standing LV failure causing RV failure.
High-output HF results from a persistently high cardiac output, which may eventually result in an inability of a normal heart to maintain adequate output. Conditions that may increase cardiac output include severe anemia, end-stage liver disease, beriberi, thyrotoxicosis, advanced Paget disease, arteriovenous fistula, and persistent tachycardia.
Cardiomyopathy is a general term indicating disease of the myocardium. Most commonly, the term refers to a primary disorder of the ventricular myocardium that is not caused by congenital anatomic defects; valvular, systemic, or pulmonary vascular disorders; isolated pericardial, nodal, or conduction system disorders; or epicardial coronary artery disease (CAD). The term is sometimes used to reflect etiology (eg, ischemic vs hypertensive cardiomyopathy). Cardiomyopathy does not always lead to symptomatic HF. It is often idiopathic and is classified as dilated, congestive, hypertrophic, infiltrative-restrictive, or apical-ballooning cardiomyopathy (also known as takotsubo or stress cardiomyopathy).
Staging of Heart Failure
International consensus defines the staging system for heart failure (HF) to highlight the need for HF prevention (1, 2):
A: High risk of HF but no structural or functional cardiac abnormalities or symptoms
B: Structural or functional cardiac abnormalities but no symptoms of HF
C: Structural heart disease with symptoms of HF
D: Refractory HF requiring advanced therapies (eg, mechanical circulatory support, cardiac transplantation) or palliative care
Clinical severity (or functional classification) varies significantly and is usually classified according to the New York Heart Association (NYHA) system (see table ); the examples of ordinary activity may be modified for older, debilitated patients. Because HF has such a broad range of severity, some experts subdivide NYHA class III into IIIA or IIIB (3, 4). Class IIIB is typically reserved for those patients who recently had a heart failure exacerbation, although the definition is not standardized.
New York Heart Association (NYHA) Functional Classification of Heart Failure
NYHA Class | Definition | Limitation | Example |
|---|---|---|---|
I | Ordinary physical activity does not cause undue fatigue, dyspnea, or palpitations | None | Can complete any activity requiring ≥ 7 METs:
|
II | Comfortable at rest; ordinary physical activity causes fatigue, dyspnea, palpitations, or angina | Mild | Can complete activity requiring ≥ 5 but ≤ 7 METs:
|
III | Comfortable at rest; less than ordinary physical activity causes fatigue, dyspnea, palpitations, or angina IIIa: Without recent HF exacerbation or recent resting dyspnea IIIb: With recent HF exacerbation or recent resting dyspnea | Moderate | Can complete activity requiring ≥ 2 and ≤ 5 METs:
|
IV | Symptomatic rest; any physical activity increases discomfort | Severe | Symptoms with all activities Cannot complete any activity requiring ≥ 2 METs (all activities listed above) |
HF = heart failure, MET = metabolic equivalent of task, a measure of how much energy is expended compared to remaining at rest; mph = mile per hour. | |||
Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines [published correction appears in J Am Coll Cardiol. 2023 Apr 18;81(15):1551. doi: 10.1016/j.jacc.2023.03.002.]. J Am Coll Cardiol. 2022;79(17):e263-e421. doi:10.1016/j.jacc.2021.12.012; Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on practice guidelines. Circulation. 2013;128(16):1810-1852. doi:10.1161/CIR.0b013e31829e8807; and Dolgin M, Association NYH, Fox AC, Gorlin R, Levin RI, New York Heart Association. Criteria Committee. Nomenclature and criteria for diagnosis of diseases of the heart and great vessels. 9th ed. Boston, MA: Lippincott Williams and Wilkins; March 1, 1994. | |||
MET values for activities are from: Herrmann SD, Willis EA, Ainsworth BE, et al. 2024 Adult Compendium of Physical Activities: A third update of the energy costs of human activities. J Sport Health Sci. 2024;13(1):6-12. doi:10.1016/j.jshs.2023.10.010 | |||
Staging references
1. Bozkurt B, Coats AJ, Tsutsui H, et al. Universal Definition and Classification of Heart Failure: A Report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition of Heart Failure. J Card Fail. Published online March 1, 2021. doi:10.1016/j.cardfail.2021.01.022
2. Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145:e895–e1032. doi: 10.1161/CIR.0000000000001062
3. Levy WC, Mozaffarian D, Linker DT, et al. The Seattle Heart Failure Model: prediction of survival in heart failure. Circulation. 2006;113(11):1424-1433. doi:10.1161/CIRCULATIONAHA.105.584102
4. Thibodeau JT, Mishkin JD, Patel PC, Mammen PP, Markham DW, Drazner MH. IIIB or not IIIB: a previously unanswered question. J Card Fail. 2012;18(5):367-372. doi:10.1016/j.cardfail.2012.01.016
Key Points
Heart failure is the inability the heart to provide tissues with adequate blood for metabolic needs.
Heart failure most commonly affects the left ventricle, but can involve the right or both ventricles.
Heart failure is classified based on the left ventricular ejection fraction into heart failure with reduced, minimally reduced, preserved, or improved ejection fraction.





