



A thorough physical examination of a newborn should be completed by a clinician within 24 hours of birth. Performing the examination with parents present allows them to ask questions and allows the clinician to point out physical findings and provide anticipatory guidance. Routine screening tests to detect problems that cannot be seen during the physical examination are also performed (see Screening Tests for Newborns).
Handwashing by all medical personnel who provide newborn care is crucial to prevent transmission of infection.
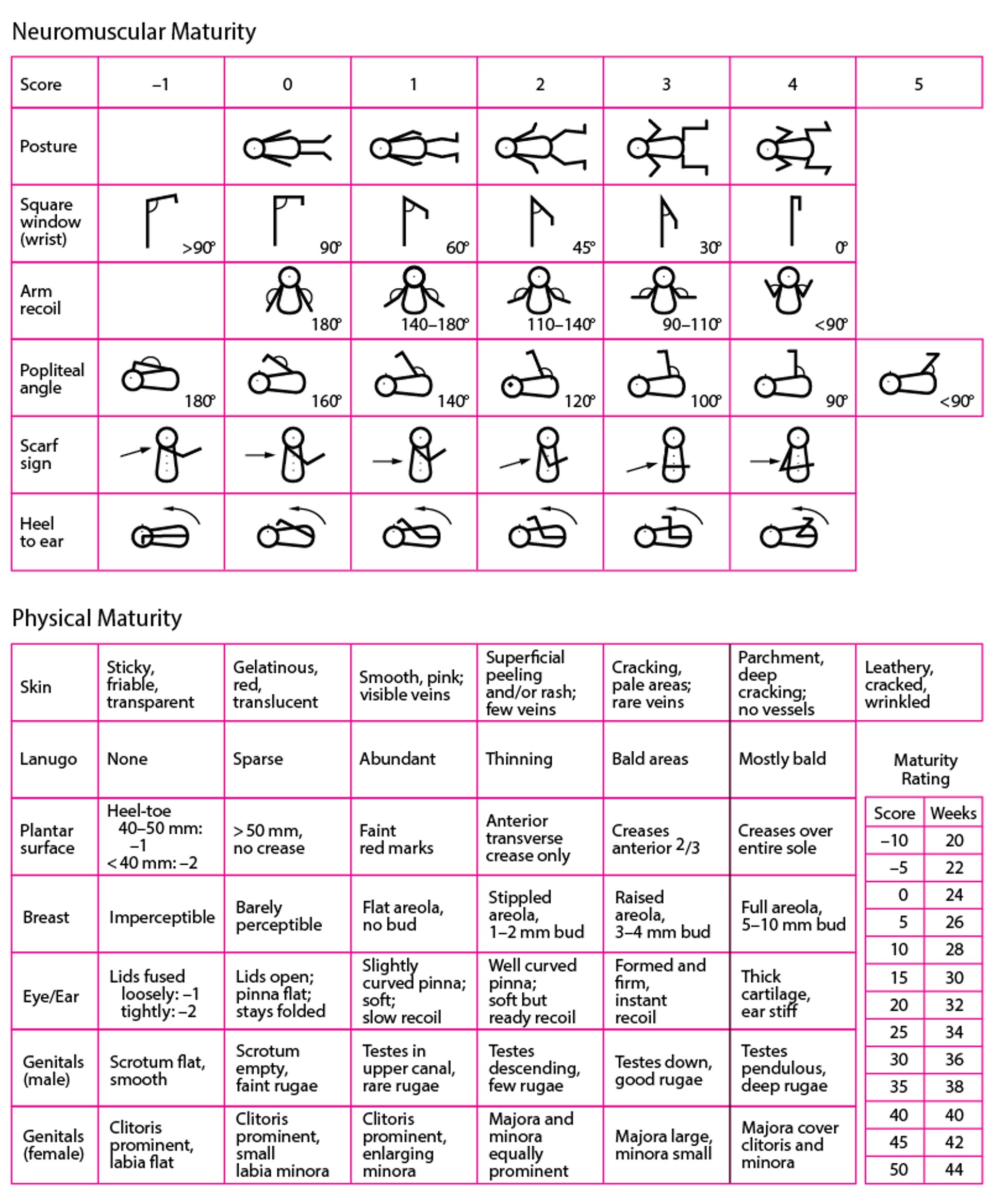
During the examination, basic measurements are taken, including length, weight, and head circumference (see also Growth Parameters in Neonates). Length is measured from crown to heel; normal values are based on gestational age and sex and should be plotted on a standard growth chart. When gestational age is uncertain or when the infant seems large for gestational age or small for gestational age, the gestational age can be more precisely determined using physical and neuromuscular findings (see figure ). These methods are typically accurate to ± 2 weeks; however, in the sick neonate these methods are less reliable.
Assessment of Gestational Age—New Ballard Score
Scores from neuromuscular and physical domains are added to obtain total score. (Adapted from Ballard JL, Khoury JC, Wedig K, et al. New Ballard score, expanded to include extremely premature infants. The Journal of Pediatrics. 1991;119(3):417–423. doi:10.1016/s0022-3476(05)82056-6; used with permission of the CV Mosby Company.) |

Many clinicians begin with examination of the heart and lungs, followed by a systematic head-to-toe examination, looking particularly for signs of birth trauma and congenital abnormalities.
Cardiorespiratory System
The heart and lungs are evaluated when the infant is quiet, often achieved by partially swaddling the infant. To avoid startling the infant, examiners should make sure their hands are not cold to the touch.
The clinician should identify where the heart sounds are loudest to exclude dextrocardia. Heart rate (normal: 100 to 160 beats/minute) and rhythm are checked. Rhythm should be regular, although an irregular rhythm from premature atrial or ventricular contractions is not uncommon. A murmur heard in the first 24 hours is most commonly caused by a patent ductus arteriosus. Daily cardiac examination confirms the disappearance of this murmur, usually within 3 days.
Femoral pulses are checked and compared with brachial pulses. Palpation of femoral pulses is particularly dependent on a calm infant, as movement or contraction of the hip and thigh muscles can make them very difficult to feel. A femoral pulse that is delayed or weak compared with the brachial pulse suggests aortic coarctation. Generally weak pulses may suggest a more proximal left ventricular outflow tract obstruction. Bounding pulses, indicating a wide pulse pressure, are consistent with a patent ductus arteriosis. Central cyanosis suggests congenital heart disease, pulmonary disease, or sepsis.
The respiratory system is evaluated by counting respirations over a full minute because breathing in neonates is irregular; normal rate is 40 to 60 breaths/minute. The chest wall should be examined for symmetry, and lung sounds should be equal throughout. Grunting, nasal flaring, and retractions are signs of respiratory distress.
(See also Congenital Cardiovascular Anomalies.)
Head and Neck
In a vertex vaginal delivery, the head is commonly molded with overriding of the cranial bones at the sutures and some swelling and ecchymosis of the scalp (caput succedaneum). In a breech delivery, the head has less molding, with swelling and ecchymosis occurring in the presenting part (ie, buttocks, genitals, or feet). The fontanelles vary in diameter from a fingertip breadth to several centimeters. A large anterior fontanelle and anything more than a fingertip breadth posterior fontanelle may be signs of hypothyroidism.
A cephalhematoma is a common finding; blood accumulates between the periosteum and the bone, producing a swelling that does not cross suture lines. It may occur over one or both parietal bones and occasionally over the occiput. Cephalhematomas usually are not evident until soft-tissue edema subsides; they gradually disappear over several months.
Inspection of head size and shape may be useful in detecting congenital hydrocephalus.
Numerous genetic syndromes cause craniofacial abnormalities. The face is inspected for symmetry and normal development, particularly of the eyes, mandible, palate, pinnae, and external auditory canals.
The eyes may be easier to examine the day after birth because the birth process causes swelling around the eyelids. Eyes should be examined for the red reflex; its absence or asymmetry may indicate glaucoma, cataracts, or retinoblastoma. Subconjunctival hemorrhages are common and caused by forces exerted during delivery.
Low-set ears may indicate genetic anomalies, including trisomy 18 and trisomy 21 (Down syndrome). Malformed ears, external auditory canals, or both may be present in many genetic syndromes. Clinicians should look for external ear pits or tags, which are sometimes associated with hearing loss and kidney abnormalities.


Image courtesy of the Centers for Disease Control and Prevention Public Health Image Library.
The clinician should inspect and palpate the palate to check for soft or hard palate defects. Orofacial clefts are among the most common congenital defects. Some neonates are born with an epulis (a benign hamartoma of the gum), which, if large enough, can cause feeding difficulties and may obstruct the airway. These lesions can be removed; they do not recur. Some neonates are born with primary or natal teeth. Natal teeth do not have roots and may need to be removed to prevent them from falling out and being aspirated. Inclusion cysts called Epstein pearls may occur on the roof of the mouth.
When examining the neck, the clinician must lift the chin to look for abnormalities such as cystic hygromas, goiters, and branchial arch remnants. Torticollis can be caused by a sternocleidomastoid hematoma due to birth trauma.
Abdomen and Pelvis
The abdomen should be round and symmetric. A scaphoid abdomen may indicate a diaphragmatic hernia, allowing the intestine to migrate through it to the chest cavity in utero; pulmonary hypoplasia and postnatal respiratory distress may result. An asymmetric abdomen suggests an abdominal mass.
The splenic edge is palpable in about 20% of newborns (1). Splenomegaly (splenic edge palpable > 2 cm below the left costal margin) suggests congenital infection or hemolytic anemia.
The kidneys may be palpable with deep palpation; the left is more easily palpated than the right. Large kidneys may indicate obstruction, tumor, or cystic disease.
The liver is normally palpable 1 to 2 cm below the costal margin. An umbilical hernia, due to a weakness of the umbilical ring musculature, is common but rarely significant. The presence of a normally placed, patent anus should be confirmed.
In boys, the penis should be examined for hypospadias or epispadias. In term boys, the testes should be in the scrotum (see Cryptorchidism). Scrotal swelling may signify hydrocele, inguinal hernia, or, more rarely, testicular torsion. With hydrocele, the scrotum transilluminates. Torsion, a surgical emergency, causes ecchymosis and firmness.
In term girls, the labia are prominent. Mucoid vaginal and serosanguineous secretions (pseudomenses) are normal; they result from exposure to maternal hormones in utero and withdrawal at birth. Attempting to visualize the hymen and its patency is important to detect vaginal obstruction. A small tag of hymenal tissue at the posterior fourchette, believed to be due to maternal hormonal stimulation, is sometimes present but disappears over a few weeks.
Ambiguous genitals (intersex) may indicate several uncommon disorders (eg, congenital adrenal hyperplasia; 5-alpha-reductase deficiency; Klinefelter syndrome, Turner syndrome, or Swyer syndrome). Referral to an endocrinologist for support with discussions with the family about benefits and risks of immediate versus delayed sex assignment can be helpful. Emergent referral to an endocrinologist is indicated if there is a concern for congenital adrenal hyperplasia since it can lead to adrenal crisis.
Abdomen and pelvis reference
1. Mimouni F, Merlob P, Ashkenazi S, Litmanovitz I, Reisner SH. Palpable spleens in newborn term infants. Clin Pediatr (Phila). 1985;24(4):197-198. doi:10.1177/000992288502400403
Musculoskeletal System
The clavicles should be palpated for crepitus to detect occult fractures. Clavicle fractures typically heal on their own. Pinning the sleeve of the affected arm to immobilize it may be recommended.
The extremities are examined for deformities, amputations (incomplete or missing limbs), contractures, and maldevelopment. Brachial nerve palsy due to birth trauma may manifest as limited or no spontaneous arm movement on the affected side, sometimes with adduction and internal rotation of the shoulder and pronation of the forearm.
The spine is inspected for signs of neural tube defects, particularly exposure of the meninges, spinal cord, or both (meningomyelocele). When present, sacral dimples are examined to determine whether the base can be visualized and for other atypical features (> 5 mm in size, > 2.5 cm from the anus, not midline) that would suggest the need for imaging or referral (1).
Orthopedic examination includes palpation of long bones for birth trauma (particularly clavicle fracture) but is focused on detection of hip dysplasia. Risk factors for dysplasia include female sex, breech position in utero, twin gestation, and family history of hip dysplasia. The Barlow and Ortolani maneuvers are used to check for dysplasia. These maneuvers must be performed when neonates are quiet. The starting position is the same for both: Neonates are placed on their back with their hips and knees flexed to 90° (the feet will be off the bed), feet facing the clinician, who places an index finger on the greater trochanter and a thumb on the lesser trochanter.
For the Barlow maneuver, the clinician adducts the hip (ie, the knee is drawn across the body) while pushing the thigh posteriorly. A felt but not heard clunk indicates that the head of the femur has moved out of the acetabulum; the Ortolani maneuver then relocates it and confirms the diagnosis.
For the Ortolani maneuver, the hip is returned to the starting position; then the hip being tested is abducted (ie, the knee is moved away from the midline toward the examining table into a frog-leg position) and gently pulled anteriorly. A palpable clunk of the femoral head with abduction signifies movement of an already dislocated femoral head into the acetabulum and constitutes a positive test for hip dysplasia.
The maneuvers may be falsely negative in infants > 3 months because of tighter hip muscles and ligaments. If the examination is abnormal or equivocal, delivery was breech, or there is a family history of developmental hip dysplasia, hip ultrasound should be performed at 2 to 6 weeks (2).


This illustration shows the Barlow maneuver (left) and the Ortolani maneuver (right), which are used to diagnose developmental dysplasia of the hip in infants. If the hip can be dislocated using the Barlow maneuver, the test is considered positive. The Ortolani maneuver is used to demonstrate that the hip has been dislocated and to reduce the dislocated hip into the acetabulum.
JEANETTE ENGQVIST/SCIENCE PHOTO LIBRARY
Musculoskeletal system references
1. Choi SJ, Yoon HM, Hwang JS, et al. Incidence of Occult Spinal Dysraphism Among Infants With Cutaneous Stigmata and Proportion Managed With Neurosurgery: A Systematic Review and Meta-analysis. JAMA Netw Open. 2020;3(7):e207221. Published 2020 Jul 1. doi:10.1001/jamanetworkopen.2020.7221
2. Mulpuri K, Song KM, Goldberg MJ, Sevarino K. Detection and Nonoperative Management of Pediatric Developmental Dysplasia of the Hip in Infants up to Six Months of Age. J Am Acad Orthop Surg. 2015;23(3):202-205. doi:10.5435/JAAOS-D-15-00006
Neurologic System
The neonate’s tone, level of alertness, movement of extremities, and reflexes are evaluated. Typically, neonatal reflexes, including the Moro, suck, and rooting reflexes, are elicited:
Moro reflex: The neonate’s response to startle is elicited by pulling the arms slightly off the bed and releasing suddenly. In response, the neonate extends the arms with fingers extended, flexes the hips, and cries.
Rooting reflex: Stroking the neonate’s cheek or lateral lip prompts the neonate to turn the head toward the touch and open the mouth.
Suck reflex: A pacifier or gloved finger is used to elicit this reflex.
These reflexes are present for several months after birth and are markers of a normal peripheral nervous system.
Axillary slippage, or feeling as if the newborn is slipping through the examiner's fingers when held upright below the arms, may indicate global hypotonia.
Skin
A neonate’s skin is usually ruddy; acrocyanosis is common in the first few hours and may persist for months, especially intermittently. Vernix caseosa covers most neonates > 24 weeks' gestation. Dryness and peeling often develop within days, especially at wrist and ankle creases.
Petechiae may occur in areas traumatized during delivery, such as the face when the face is the presenting part; however, neonates with diffuse petechiae should be evaluated for thrombocytopenia and serious infection.
Many neonates have erythema toxicum, a benign rash with an erythematous base and a white or yellow papule. This rash, which usually appears 24 hours after birth, is scattered over the body and can last for up to 2 weeks.


This photo shows erythema toxicum, a benign rash with an erythematous base and a white or yellow papule.
© Springer Science+Business Media





