

Pericarditis is inflammation of the pericardium , often with fluid accumulation in the pericardial space. Pericarditis may be caused by many disorders (eg, infection, myocardial infarction, trauma, tumors, metabolic disorders) but is often idiopathic. Symptoms include chest pain or tightness, often worsened by deep breathing. Cardiac output may be greatly reduced if cardiac tamponade or constrictive pericarditis develops. Diagnosis is based on symptoms, a friction rub, electrocardiographic changes, and evidence of pericardial effusion or inflammation on imaging or laboratory tests. Finding the cause requires further evaluation. Treatment depends on the cause, but general measures include analgesics, anti-inflammatory medications, colchicine, and rarely surgery.
Pericarditis is the most common pericardial disorder. Other pericardial disorders include pericardial effusion, constrictive pericarditis, fibrosis of the pericardium. Congenital pericardial disorders are rare.
Anatomy of the Pericardium
The pericardium is a fibroserous sac surrounding the heart and the proximal portions of the great vessels. The pericardium has 2 layers (1). The visceral pericardium is a single layer of mesothelial cells that is attached to the myocardium, folds back (reflects) on itself over the origin of the great vessels, and joins with a tough, fibrous layer to envelop the heart as the parietal pericardium. The sac created by these layers contains a small amount of fluid (< 25 to 50 mL), composed mostly of an ultrafiltrate of plasma.
Physiology of the pericardium
The pericardium limits acute cardiac distention, lubricates the outer surface of the heart during cardiac contraction, enhances the mechanical interactions of the cardiac chambers, and moderates cardiopulmonary interactions (2). The pericardium also provides a mechanical immunologic barrier for the heart. The pericardium is richly innervated with sympathetic and somatic afferents. Stretch-sensitive mechanoreceptors sense changes in cardiac volume and tension and may be responsible for transmitting pericardial pain. The phrenic nerves are embedded in the parietal pericardium and are vulnerable to injury during surgery on the pericardium.
Anatomy references
1. Hoit BD. Anatomy and Physiology of the Pericardium. Cardiol Clin. 2017;35(4):481-490. doi:10.1016/j.ccl.2017.07.002
2. Wang TKM, Klein AL, Cremer PC, et al. 2025 Concise Clinical Guidance: An ACC Expert Consensus Statement on the Diagnosis and Management of Pericarditis: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2025;86(25):2691-2719. doi:10.1016/j.jacc.2025.05.023
Pathophysiology of Pericarditis
Pericarditis may be (1):
Acute (symptoms ≤ 4 weeks)
Subacute (symptoms > 4 weeks to ≤ 3 months)
Chronic (symptoms > 3 months)
Acute pericarditis develops quickly, causing inflammation of the pericardial sac and often a pericardial effusion. Inflammation can extend to the epicardial myocardium (myopericarditis). Adverse hemodynamic effects and rhythm disturbances are rare, although cardiac tamponade is possible.
Acute disease may resolve completely, resolve and reoccur (up to 30% of acute cases) or become subacute or chronic (2). These forms develop more slowly.
Subacute pericarditis occurs within weeks to months of an inciting event and may resolve spontaneously or with medical therapy.
Incessant pericarditis lasts longer than 4 to 6 weeks without remission (3).
Recurrent pericarditis is used to describe pericarditis that returns after a 4 to 6 week symptom-free interval.
Chronic pericarditis is defined as pericarditis persisting > 3 months.
Pericardial effusion is accumulation of fluid in the pericardium. The fluid may be serous fluid (sometimes with fibrin strands), serosanguineous fluid, blood, pus, or chyle.
Cardiac tamponade occurs when a moderate or large pericardial effusion impairs cardiac filling, leading to low cardiac output and sometimes shock and death. If fluid (usually blood) accumulates rapidly, even small amounts (eg, 150 mL) may cause tamponade because the pericardium cannot stretch quickly enough to accommodate it. Conversely, slow accumulation of up to 1500 mL may not cause tamponade. Loculated effusion may cause localized tamponade on the right or left side of the heart and may be difficult to diagnose.
Constrictive pericarditis
Occasionally, pericarditis causes constrictive pericarditis, a marked thickening and stiffening of the pericardium. Constrictive pericarditis results from marked inflammatory, fibrotic thickening of the pericardium. Sometimes the visceral and parietal layers adhere to each other or to the myocardium. The fibrotic tissue often contains calcium deposits. The stiff, thickened pericardium markedly impairs ventricular filling, decreasing stroke volume and cardiac output. Significant pericardial fluid accumulation is rare. Rhythm disturbance is common, particularly atrial fibrillation. The diastolic pressures in the ventricles, atria, and venous beds become virtually the same. Systemic venous congestion occurs, causing considerable transudation of fluid from systemic capillaries, with dependent edema and, later, ascites. Chronic elevation of systemic venous pressure and hepatic venous pressure may lead to liver scarring, called cardiac cirrhosis, in which case, patients may initially present for evaluation of cirrhosis. Constriction of the left atrium, the left ventricle, or both may elevate pulmonary venous pressure. Occasionally, pleural effusion develops.
There are several variants of constrictive pericarditis:
Subacute (early stage) constrictive pericarditis, developing weeks to months after an inciting injury and managed initially with medical therapy
Transient constrictive pericarditis (typically subacute) is that which resolves spontaneously or after medical therapy
Chronic constrictive pericarditis, usually requiring pericardiectomy as definitive treatment
Effusive-constrictive pericarditis characterized by pericardial constriction involving the visceral pericardium with significant pericardial effusion sometimes requiring treatment for cardiac tamponade
Pathophysiology references
1. Schulz-Menger J, Collini V, Gröschel J, et al. 2025 ESC Guidelines for the management of myocarditis and pericarditis. Eur Heart J. 2025;46(40):3952-4041. doi:10.1093/eurheartj/ehaf192
2. Imazio M, Gaita F, LeWinter M. Evaluation and Treatment of Pericarditis: A Systematic Review [published correction appears in JAMA. 2015 Nov 10;314(18):1978] [published correction appears in JAMA. 2016 Jan 5;315(1):90. Dosage error in article text]. JAMA. 2015;314(14):1498-1506. doi:10.1001/jama.2015.12763
3. Wang TKM, Klein AL, Cremer PC, et al. 2025 Concise Clinical Guidance: An ACC Expert Consensus Statement on the Diagnosis and Management of Pericarditis: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2025;86(25):2691-2719. doi:10.1016/j.jacc.2025.05.023
Etiology of Pericarditis
Acute pericarditis may result from infection, autoimmune or inflammatory disorders, uremia, injury or surgery, myocardial infarction (MI), cancer, radiation therapy, or certain medications (see table ).
Infectious pericarditis is most often viral or idiopathic (often presumed to be viral) in North America and Western Europe (1). Tuberculosis, on the other hand, is the most common cause in regions where it is endemic. Purulent bacterial pericarditis is uncommon but may follow infective endocarditis, pneumonia, septicemia, penetrating trauma, or cardiac surgery. Often, the cause cannot be identified (called nonspecific or idiopathic pericarditis), but many of these cases are probably viral.
Pericarditis can occur during or after acute myocardial infarction (MI), in two distinct clinical syndromes. Early post-myocardial infarction pericarditis (or peri-infarction pericarditis) occurs immediately after MI; its incidence in one cohort was 1 to 2 % of MI patients, with a gradual decrease in incidence from 2000 to 2013 (2). Post-myocardial infarction syndrome (Dressler syndrome) is a less common cause, typically occurring more than one week after MI when reperfusion with percutaneous transluminal coronary angioplasty (PTCA) or thrombolytic medications is ineffective in patients with transmural infarction (3). Post-MI syndrome has become exceedingly rare, and may have vanished, in the current era of early reperfusion and standardized post-MI medical therapy (4).
Pericarditis occurs after pericardiotomy (called postpericardiotomy syndrome) in 5 to 30% of cardiac operations (5). Postpericardiotomy syndrome, traumatic pericarditis (which includes iatrogenic pericarditis, after, eg, percutaneous cardiac intervention, pacemaker placement, and ablation), and post-MI syndrome comprise the post-cardiac injury syndrome.
Causes of Acute Pericarditis
Cause | Examples |
|---|---|
Infections | |
Bacterial infections | Haemophilus influenzae (in children) Rheumatic fever |
Viral infections | Coxsackie B virus Echovirus HIV† |
Fungal infections | |
Parasitic infections | |
Pericardial injury | |
Trauma | — |
Postpericardiotomy syndrome | — |
Radiation therapy | — |
— | |
— | |
Systemic disease | |
Systemic rheumatic diseases | |
Inflammatory disorders | Myocarditis with pericardial involvement Rheumatic fever |
Cancer | Kaposi sarcoma (in people with HIV infection) |
Uremia | — |
Hypothyroidism | — |
Other | |
Medications | Anticoagulants HydralazineHydralazine Immune checkpoint inhibitors IsoniazidIsoniazid Methysergide Penicillin PhenytoinPhenytoin ProcainamideProcainamide |
Congenital absence or abnormality of the pericardium | — |
Idiopathic | — |
* Tuberculous pericarditis accounts for a small percentage of cases of acute or subacute pericarditis in North America and Western Europe but the majority of cases are in endemic areas of India and Africa. | |
† If patients with HIV infection develop lymphoma, Kaposi sarcoma, or certain infections (eg, Mycobacterium avium, M. tuberculosis, or Nocardia infections; other fungal or viral infections), pericarditis may follow. | |
Bendjelid K, Pugin J. Is Dressler syndrome dead?. Chest. 2004;126(5):1680-1682. doi:10.1378/chest.126.5.1680 and Wang TKM, Klein AL, Cremer PC, et al. 2025 Concise Clinical Guidance: An ACC Expert Consensus Statement on the Diagnosis and Management of Pericarditis: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2025;86(25):2691-2719. doi:10.1016/j.jacc.2025.05.023 | |
Subacute pericarditis is a prolongation of acute pericarditis and thus has the same causes. Some patients have transient constriction occurring days to weeks after recovery from acute pericarditis.
Chronic effusive pericarditis or chronic constrictive pericarditis may follow acute pericarditis of almost any etiology. In high-resource areas, the most common antecedents of constrictive pericarditis are similar to those of acute pericarditis: idiopathic/viral, prior cardiac surgery, and history of radiation therapy; worldwide, the most common cause is tuberculous pericarditis (6). In addition, some cases occur without antecedent acute pericarditis.
Chronic pericarditis with a large effusion (serous, serosanguineous, or bloody) is most commonly caused by metastatic tumors (7), most often by lung carcinoma, breast carcinoma, sarcoma, melanoma, leukemia, or lymphoma.
Hypothyroidism may cause pericardial effusion and cholesterol pericarditis. Cholesterol pericarditis is a rare disorder that may be associated with hypothyroidism or other chronic inflammatory diseases, in which ongoing inflammation and a chronic pericardial effusion allow cholesterol crystals to accumulate in the pericardial space, leading to a elevated pericardial cholesterol levels that further drive inflammation and worsen pericarditis.
Sometimes no cause of chronic pericarditis is identified.
Transient constrictive pericarditis is most commonly caused by infection or postpericardiotomy inflammation or is idiopathic.
Fibrosis of the pericardium, sometimes leading to chronic constrictive pericarditis, may follow purulent pericarditis or accompany a systemic rheumatic disease. In older patients, common causes are malignant tumors, myocardial infarction, and tuberculosis.
Hemopericardium (accumulation of blood within the pericardium) may lead to pericarditis or pericardial fibrosis; common causes include chest trauma, iatrogenic injury (eg, resulting from cardiac catheterization, pacemaker insertion, central venous line placement), and rupture of a thoracic aortic aneurysm.
Etiology references
1. Cremer PC, Klein AL, Imazio M. Diagnosis, Risk Stratification, and Treatment of Pericarditis: A Review. JAMA. 2024;332(13):1090-1100. doi:10.1001/jama.2024.12935
2. Lador A, Hasdai D, Mager A, et al. Incidence and Prognosis of Pericarditis After ST-Elevation Myocardial Infarction (from the Acute Coronary Syndrome Israeli Survey 2000 to 2013 Registry Database). Am J Cardiol. 2018;121(6):690-694. doi:10.1016/j.amjcard.2017.12.006
3. Shahar A, Hod H, Barabash GM, Kaplinsky E, Motro M. Disappearance of a syndrome: Dressler's syndrome in the era of thrombolysis. Cardiology. 1994;85(3-4):255-258. doi:10.1159/000176683
4. Bendjelid K, Pugin J. Is Dressler syndrome dead?. Chest. 2004;126(5):1680-1682. doi:10.1378/chest.126.5.1680
5. Lehto J, Kiviniemi T. Postpericardiotomy syndrome after cardiac surgery. Ann Med. 2020;52(6):243-264. doi:10.1080/07853890.2020.1758339
6. Janus SE, Hoit BD. Effusive-constrictive pericarditis in the spectrum of pericardial compressive syndromes [published correction appears in Heart. 2021 Nov;107(22):e17]. Heart. Published online January 15, 2021. doi:10.1136/heartjnl-2020-316664
7. Corey GR, Campbell PT, Van Trigt P, et al. Etiology of large pericardial effusions. Am J Med. 1993;95(2):209-213. doi:10.1016/0002-9343(93)90262-n
Symptoms and Signs of Pericarditis
Some patients present with symptoms and signs of inflammation (acute pericarditis); others present with those of fluid accumulation (pericardial effusion) or constriction.
Symptoms and signs vary depending on the severity of inflammation and the amount and rate of fluid accumulation. Even a large amount of pericardial fluid may be asymptomatic if it develops slowly (eg, over months).
Acute pericarditis
The classic symptoms and signs of acute pericarditis are pleuritic chest pain, fever, and a pericardial rub, and sometimes dyspnea. The first evidence can be tamponade, with hypotension, shock, or pulmonary edema
Because the innervation of the pericardium and myocardium is the same, the chest pain of pericarditis is sometimes similar to that of myocardial inflammation or ischemia: Dull or sharp precordial or substernal pain may radiate to the neck, trapezius ridge (especially the left), or shoulders. Pain ranges from mild to severe. Unlike chest pain due to ischemia, pain due to pericarditis is usually aggravated by thoracic motion, cough, breathing, or swallowing food; it may be relieved by sitting up and leaning forward.
Tachypnea and nonproductive cough may be present; fever, chills, and weakness are common. In 15 to 30% of patients with idiopathic pericarditis, symptoms recur after the initial episode (1).
The most important physical finding is a triphasic or a systolic and diastolic precordial friction rub. However, the rub is often intermittent and evanescent; it may be present only during systole or, less frequently, only during diastole. Sometimes, a pleural component to the rub is noted during breathing, which is due to inflammation of the pleura adjacent to the pericardium.

Pericardial effusion
Pericardial effusion is often painless, but when it occurs with acute pericarditis, pain may be present. Considerable amounts of pericardial fluid may muffle heart sounds, increase the area of cardiac dullness, and change the size and shape of the cardiac silhouette. A pericardial rub may be heard. With large effusions, compression of the base of the left lung can decrease breath sounds (heard near the left scapula) and cause crackles. Arterial pulse, jugular venous pulse, and blood pressure are normal unless intrapericardial pressure increases substantially, causing tamponade.
In post-MI syndrome, pericardial effusion can occur with fever, friction rub, pleural inflammation, pleural effusions, and joint pain. This syndrome usually occurs within 10 days to 2 months after MI. It is usually mild but may be severe. Occasionally, the heart ruptures post-MI, causing hemopericardium and tamponade, usually 1 to 10 days post-MI and more commonly in females.
Cardiac tamponade
The clinical findings of cardiac tamponade, also called pericardial tamponade, are similar to those of cardiogenic shock: decreased cardiac output, low systemic arterial pressure, tachycardia, and dyspnea. However, neck veins are markedly dilated. Severe cardiac tamponade is nearly always accompanied by a fall of > 10 mm Hg in systolic blood pressure during inspiration (pulsus paradoxus). In advanced cases, pulse may disappear during inspiration. (However, pulsus paradoxus can also occur in chronic obstructive pulmonary disease [COPD], bronchial asthma, pulmonary embolism, right ventricular infarction, and noncardiogenic shock.) Heart sounds are muffled unless the effusion is small. Echocardiographic findings can suggest cardiac tamponade although the diagnosis remains clinical. Loculated effusions and eccentric or localized hematoma may cause localized tamponade, in which only selected cardiac chambers are compressed. In these cases, physical, hemodynamic, and some echocardiographic signs may be absent. (See also Cardiac tamponade due to trauma.)
Constrictive pericarditis
Fibrosis or calcification rarely causes symptoms unless constrictive pericarditis develops. The only early abnormalities may be elevated ventricular diastolic, atrial, pulmonary, and systemic venous pressures. Symptoms and signs of peripheral venous congestion (eg, peripheral edema, neck vein distention, hepatomegaly) may appear with an early diastolic sound (pericardial knock), often best heard during inspiration. This sound is due to abrupt slowing of diastolic ventricular filling by the rigid pericardium.
Ventricular systolic function (based on ejection fraction) is usually preserved. Prolonged elevation of pulmonary venous pressure results in dyspnea (particularly during exertion) and orthopnea. Fatigue may be severe. Distention of neck veins with a rise in venous pressure during inspiration (Kussmaul sign) is present; it is absent in tamponade. Pulsus paradoxus is rare and is usually less severe than in tamponade. Lungs are not congested unless severe left ventricular constriction develops.
Symptoms and signs reference
1. Wang TKM, Klein AL, Cremer PC, et al. 2025 Concise Clinical Guidance: An ACC Expert Consensus Statement on the Diagnosis and Management of Pericarditis: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2025;86(25):2691-2719. doi:10.1016/j.jacc.2025.05.023
Diagnosis of Pericarditis
History and physical examination
Electrocardiography (ECG)
Echocardiography, cardiac MRI, cardiac CT
Tests to identify cause (eg, chest radiograph or CT, pericardial fluid aspiration, pericardial biopsy)
ECG is performed to evaluate for characteristic ECG changes. Echocardiography is performed to check for effusion, cardiac filling abnormalities that may suggest cardiac tamponade, and wall motion abnormalities characteristic of myocardial involvement. Cardiac MRI may be performed to evaluate for myopericardial edema/inflammation. Cardiac CT can evaluate pericardial thickness and calcification as well as identify constrictive physiology. Chest radiograph or CT scan may be performed to evaluate the cause of the presenting symptoms or to determine the cause of pericarditis once suspected. Blood tests may detect leukocytosis and elevated markers of inflammation (eg, C-reactive protein [CRP], erythrocyte sedimentation rate [ESR]), which may be used in diagnosis or to guide duration of therapy.
Acute pericarditis
Diagnostic criteria
Classically, the diagnosis of acute pericarditis has been based on the presence of ≥ 2 of 4 features: characteristic chest pain, pericardial friction rub, ECG abnormalities, and pericardial effusion (1, 2). Subsequent diagnostic criteria distinguish definite, possible, and unlikely/rejected pericarditis (3, 4). In the setting of a typical clinical presentation (pleuritic chest pain or an equivalent finding), the number of additional diagnostic findings determines the diagnosis:
Definite pericarditis: Typical clinical presentation with ≥ 2 diagnostic findings
Possible pericarditis: Typical clinical presentation with 1 diagnostic finding
Unlikely/rejected pericarditis: Typical clinical presentation with no diagnostic finding
The additional diagnostic findings used for these diagnostic criteria are:
Examination: Pericardial friction rub
ECG: Diffuse PR depression and/or ST elevation
Inflammatory markers: Elevated C-reactive protein or erythrocyte sedimentation rate
Echocardiography (or other imaging): New or worsening pericardial effusion
Cardiac MRI: Pericardial edema or late gadolinium enhancement
The time course can be further classified as acute, incessant, recurrent, or chronic (see Pathophysiology).
Testing
Serial ECGs may be needed to show abnormalities. The ECG in acute pericarditis may show abnormalities confined to ST and PR segments and T waves, usually in most leads. (ECG changes in lead aVR are generally in the opposite direction of other leads.) Unlike myocardial infarction, acute pericarditis does not cause reciprocal depression in ST segments (except in leads aVR and V1), and there are no pathologic Q waves. ECG changes in pericarditis can occur in 4 stages although not all stages are present in all cases.
Acute Pericarditis: Stage 1 ECG
J points, except aVR and V1, are elevated. T waves are essentially normal. ST segments show upward concave elevation. PR segments, except aVR and V1, are depressed. PR deviations are commonly absent in one limb lead (here, aVL). |

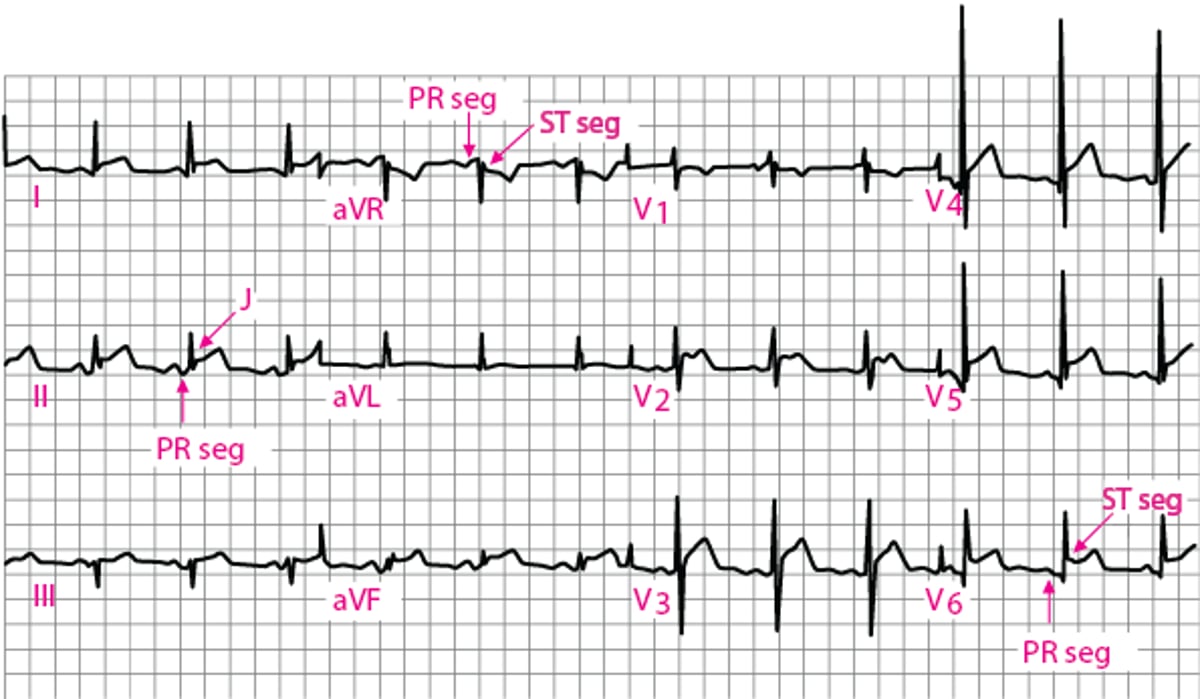
Stage 1: ST segments show upward concave elevation; the PR segments may be depressed (see figure ).
Stage 2: ST segments return to baseline; T waves flatten.
Stage 3: T waves are inverted throughout the ECG; T wave–inversion occurs after the ST segment has returned to baseline and thus differs from the pattern of acute ischemia or MI.
Stage 4: T wave changes resolve.
Echocardiography in acute pericarditis typically shows an effusion, except in patients with purely fibrinous acute pericarditis in whom echocardiography is often normal. Findings indicating myocardial involvement include new focal or diffuse left ventricular dysfunction or abnormal strain.
Cardiac MRI can detect the presence, severity, and acuity of pericardial inflammation and can help establish the diagnosis of acute pericarditis. MRI can also identify extension of inflammation into the subjacent myocardium (myopericarditis), which occurs in up to 15 to 24% of cases (5). Unlike myocarditis or perimyocarditis (prevalent myocarditis with pericardial extension), there is no identified adverse long-term outcome.
Differential diagnosis
Because the pain of pericarditis may resemble that of acute MI or pulmonary infarction, additional tests (eg, serum cardiac biomarker measurement, CT angiography) may be required if the history and ECG findings are atypical for pericarditis. Troponin is often elevated in acute pericarditis due to epicardial inflammation, so it cannot discriminate between pericarditis, acute infarction, and pulmonary embolism. Very high levels of troponin may indicate myopericarditis.
Postpericardiotomy and post-MI syndromes may be difficult to identify and must be distinguished from recent MI, pulmonary embolism, and pericardial infection after surgery. Pain, friction rub, and fever appearing 2 weeks to several months after surgery and a rapid response to aspirin, nonsteroidal anti-inflammatory drugs (NSAIDs), colchicine, or glucocorticoids are suggestive of post-injury pericarditis.Postpericardiotomy and post-MI syndromes may be difficult to identify and must be distinguished from recent MI, pulmonary embolism, and pericardial infection after surgery. Pain, friction rub, and fever appearing 2 weeks to several months after surgery and a rapid response to aspirin, nonsteroidal anti-inflammatory drugs (NSAIDs), colchicine, or glucocorticoids are suggestive of post-injury pericarditis.
Pericardial effusion
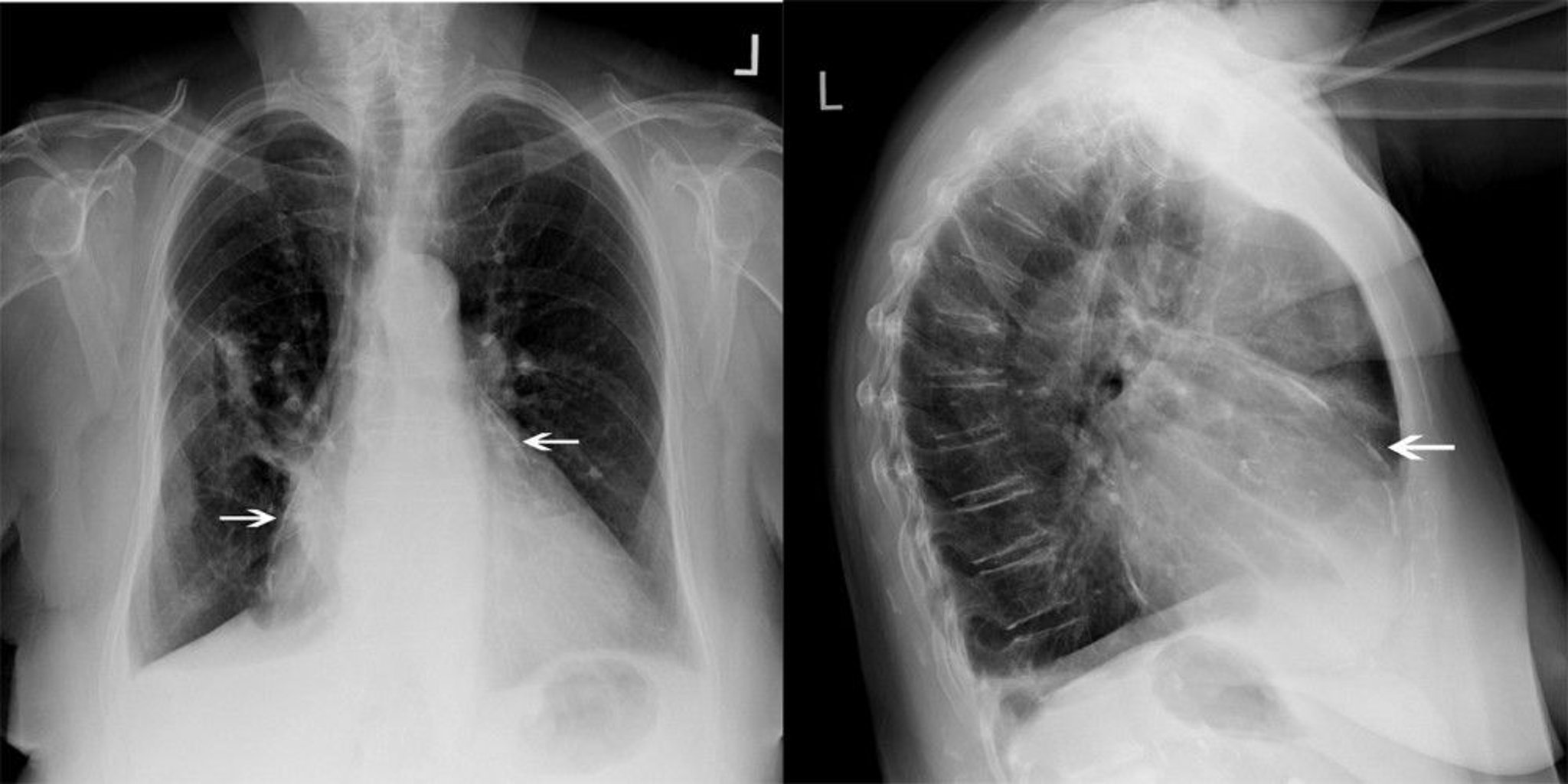
Diagnosis of pericardial effusion may be suggested by clinical findings but often is suspected after finding an enlarged cardiac silhouette on chest radiograph. On ECG, QRS voltage is often decreased, and sinus rhythm remains in most patients. With large, chronic effusions, the ECG may show electrical alternans (ie, P, QRS, or T wave amplitude increases and decreases on alternate beats). Electrical alternans is associated with variation in cardiac position (swinging heart).


This radiograph shows enlarged cardiac silhouette in a patient with a pericardial effusion.
© 2017 Elliot K. Fishman, MD.
Echocardiography typically confirms the diagnosis and estimates the size of pericardial effusion; helps to identify cardiac tamponade and myocardial dysfunction suggestive of myocarditis and/or heart failure; and may suggest the cause of pericarditis.
Although CT can detect a pericardial effusion (often incidentally on a scan performed for other conditions), it may overestimate its size and is not a first-line test to evaluate possible pericardial effusion. Cardiac MRI can also identify a pericardial effusion and may be performed as part of the diagnostic evaluation of pericarditis or myocarditis.
Patients with a normal ECG, small (< 1 cm on echocardiogram, or 100 mL) effusion, and no suspicious findings from the history and examination may be observed with serial examination and echocardiography. Other patients must be evaluated further to determine etiology.
Cardiac tamponade
Low voltage and electrical alternans on the ECG suggest cardiac tamponade, but these findings lack sensitivity and specificity (6). When tamponade is suspected, echocardiography is performed unless even a brief delay might be life threatening. Then pericardiocentesis is performed immediately for diagnosis and treatment. Echocardiographic findings that support tamponade include the following (7):
Exaggerated respiratory variation of transvalvular and venous flows
Compression or collapse of right cardiac chambers in the presence of a pericardial effusion
Inferior vena caval plethora (decrease in the proximal vena caval diameter by < 50% during deep inspiration)
However, cardiac tamponade is primarily a clinical diagnosis.
Pearls & Pitfalls
|
If tamponade is suspected but not yet confirmed (eg, by clinical findings and echocardiography), right heart (Swan-Ganz) catheterization may be performed. In cardiac tamponade:
There is no early diastolic dip in the ventricular pressure record.
Diastolic pressures are elevated (approximately 10 to 30 mm Hg) and equal in all cardiac chambers and in the pulmonary artery.
In the atrial pressure curve, x descent is preserved and y descent is lost.
In contrast, in severe congestive states due to dilated cardiomyopathy or pulmonary artery occlusion, left ventricular diastolic pressure usually exceeds right atrial mean pressure and right ventricular diastolic pressure by ≥ 4 mm Hg.
Right heart catheterization should be considered when draining an effusion, not only to confirm tamponade, but also to uncover possible constrictive pericarditis with effusion.
Diagnosis of cause
After pericarditis is diagnosed, tests to determine etiology and the effect on cardiac function are performed. In a young, previously healthy adult who presents with a viral infection and acute pericarditis, an extensive evaluation is usually unnecessary. Differentiating viral from idiopathic pericarditis is difficult, can involve extensive testing, and generally is of little practical importance.
In other cases, a biopsy of pericardial tissue or aspiration of pericardial fluid may be needed to establish a diagnosis. Acid-fast stains and cultures of pericardial fluid are essential if tuberculosis (TB) is considered possible (TB pericarditis can be aggressive and can worsen rapidly with glucocorticoid therapy). Samples are examined for malignant cells. Persistent (usually > 3 months) or progressive effusion, particularly when the etiology is uncertain, also warrants pericardiocentesis. The choice of needle pericardiocentesis versus surgical drainage for diagnostic sampling depends upon institutional resources and physician experience, the etiology of the effusion, the need for diagnostic tissue samples, and the patient's disease severity, particularly the presence of tamponade. Needle pericardiocentesis is often best when the etiology is known or the presence of tamponade is in question. Surgical drainage is best when the presence of tamponade is certain but (because pericardial biopsy can be performed surgically) the etiology is unclear.
Laboratory test results of pericardial fluid other than culture and cytology are usually nonspecific. But specific diagnoses are sometimes possible using visual, cytologic, and immunologic analysis of fluid obtained via pericardioscopic-guided biopsy.
Cardiac catheterization may be useful for evaluating pericarditis and identifying the cause of reduced cardiac function.
CT or MRI can help identify metastases.
Other tests include complete blood count, acute-phase reactants, routine chemistry tests, cultures, autoimmune tests, and, when appropriate, tests for HIV, histoplasmosis complement fixation (in endemic areas), and antibody tests for coxsackievirus, influenza virus, echovirus, and streptococcus. Nucleic acid antibody tests (including polymerase chain reaction) may be useful. A tuberculin skin test (usually PPD) or interferon gamma release assay is performed, but these tests can give false-negative results; TB pericarditis can be diagnosed or excluded only by culture of pericardial fluid for acid-fast bacilli.
Constrictive pericarditis
Constrictive pericarditis is generally a long-term, rather than acute, complication of pericarditis.
Diagnosis may be suspected based on clinical, ECG, chest radiograph, and echocardiographic or cardiac MRI findings, but cardiac catheterization and CT are often useful to confirm the diagnosis, particularly in patients with nondiagnostic echocardiograms, and to assist in perioperative management. Rarely, right heart biopsy is needed to exclude restrictive cardiomyopathy.
ECG changes are nonspecific. QRS voltage is usually low. T waves are usually nonspecifically abnormal. Atrial fibrillation occurs in about some patients; atrial flutter is less common.
Lateral chest radiograph often shows pericardial calcification best, but the finding is nonspecific.

This patient with constrictive pericarditis has significant pericardial calcification (white arrows).
© 2017 Elliot K. Fishman, MD.
Echocardiography also is nonspecific. When the right and left ventricular filling pressures are equally elevated, Doppler echocardiography helps distinguish constrictive pericarditis from restrictive cardiomyopathy.
During inspiration, mitral diastolic flow velocity usually falls > 25% in constrictive pericarditis but < 15% in restrictive cardiomyopathy.
In constrictive pericarditis, inspiratory tricuspid flow velocity increases more than it normally does, but it does not do so in restrictive cardiomyopathy.
Determining tissue velocities (measured by applying the Doppler principle to tissue motion as opposed to blood flow) at the mitral annulus may be helpful when excessively high left atrial pressure blunts respiratory variation in transvalvular velocities. Mitral annular tissue velocities (referred to as e'), especially at the septal location, increase in constrictive pericarditis and decrease in restrictive cardiomyopathy. Annulus reversus, a condition in which the septal e' velocity is greater than the lateral e' velocity, is highly specific for the presence of constrictive pericarditis (8). A shift of the interventricular septum toward the left ventricle during inspiration and away from the left ventricle during expiration and hepatic vein expiratory diastolic flow reversal (which occurs due to a dissociation of intracardiac and intrathoracic pressures and enhanced ventricular interaction) can also be visible in constrictive pericarditis.
Respiration-related ventricular septal shift, a restrictive mitral inflow pattern with respiratory variation, preserved or increased medial annular velocity, annulus reversus, and hepatic vein expiratory diastolic flow reversal collectively are referred to as the Mayo criteria (9). These variables were validated and showed that a septal shift in combination with either increased medial annular tissue velocities or hepatic expiratory diastolic flow reversals resulted in optimal sensitivity (87%) and specificity (91%) for the diagnosis of constrictive pericarditis (9, 10). Vena caval enlargement (plethora) reflects elevated venous pressure.
Cardiac catheterization, right and left sided, is performed if clinical and echocardiographic findings suggest constrictive pericarditis. Cardiac catheterization helps confirm and quantify the abnormal hemodynamics that define constrictive pericarditis:
Mean pulmonary artery occlusion pressure (pulmonary capillary wedge pressure), pulmonary artery diastolic pressure, right ventricular end-diastolic pressure, and mean right atrial pressure are roughly equal, all at approximately 10 to 30 mm Hg.
The pulmonary artery and right ventricular systolic pressures are normal or modestly elevated, so that pulse pressures are small.
In the atrial pressure curve, x and y descents are typically accentuated.
In the ventricular pressure curve, a diastolic dip occurs at the time of rapid ventricular filling.
During peak inspiration, right ventricular pressure increases when left ventricular pressure is lowest (sometimes called mirror-image discordance, suggesting increased ventricular interdependence).
Because ventricular filling is restricted, ventricular pressure tracings show a sudden dip followed by a plateau (resembling a square root sign) in early diastole.
Simultaneous recordings of right and left ventricle pressures demonstrate discordant variation of the systolic waveforms during respiration, unlike the concordant variation occurring in other causes of heart failure.
Measuring these changes requires simultaneous right and left heart cardiac catheterization, using separate transducers. These hemodynamic changes almost always occur with significant constrictive pericarditis, but changes may be masked during hypovolemia.
Right ventricular systolic pressure of > 50 mm Hg often occurs in restrictive cardiomyopathy but less often in constrictive pericarditis. When the pulmonary artery occlusion pressure equals the right atrial mean pressure and an early diastolic dip in the ventricular pressure curve occurs with large x and y waves in the right atrial curve, either disorder may be present.
CT and MRI are both useful in diagnosing constrictive pericarditis. CT offers greater spatial resolution for pericardial thickening, and MR offers more definitive diagnostic information on constrictive physiology and hemodynamics (5). Specific diagnostic features seen on cross-sectional imaging include:
Pericardial thickening > 4-mm, with typical hemodynamic changes (assessed by echocardiography and catheterization), can confirm constrictive pericarditis .
When no pericardial thickening or fluid is seen, the diagnosis of restrictive cardiomyopathy is favored but not proved.
A normal pericardial thickness does not exclude constrictive pericarditis.
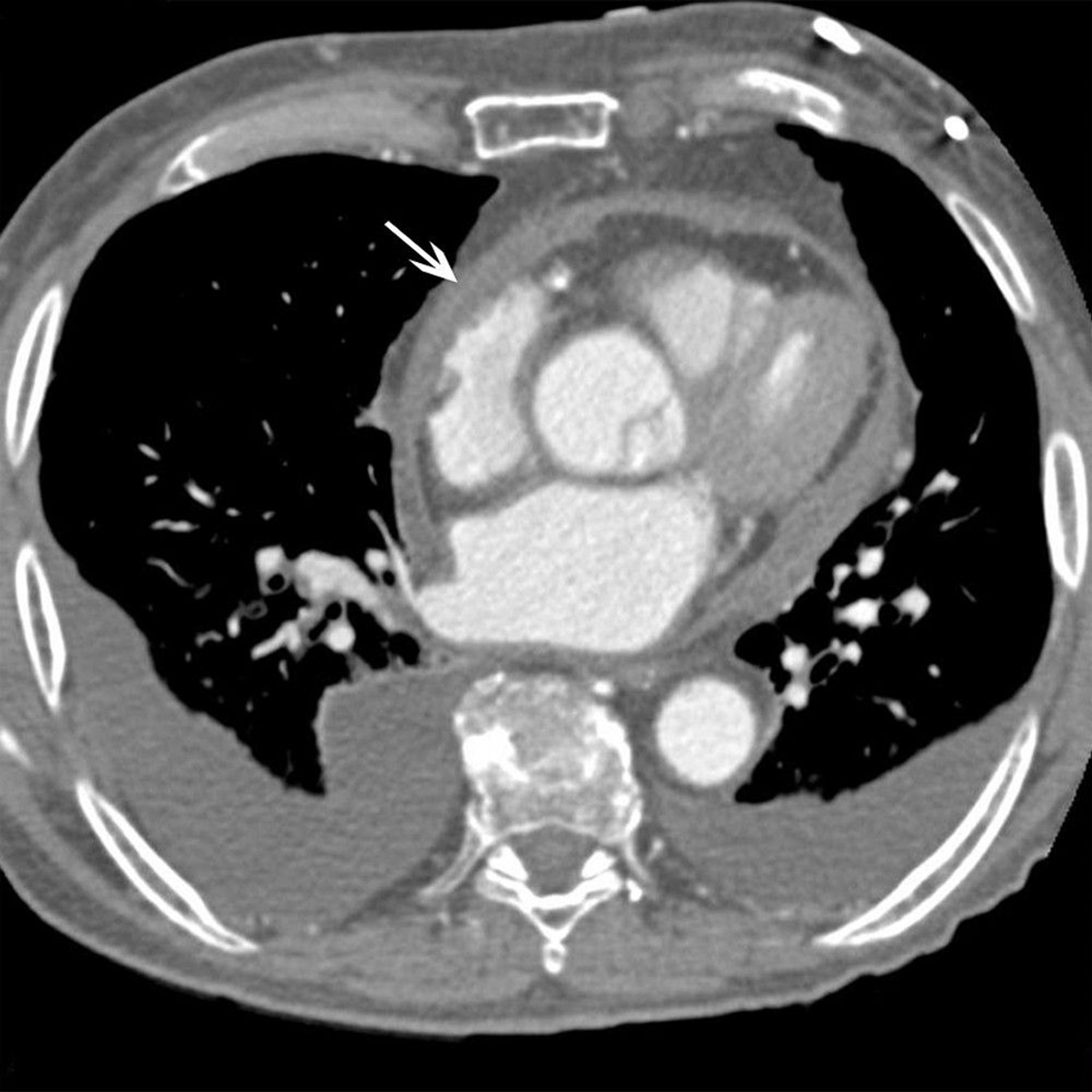
This patient with constrictive pericarditis has significant pericardial thickening on CT scan (white arrow).
© 2017 Elliot K. Fishman, MD.
Cardiac MRI can help identify chronic constrictive pericarditis that is unlikely to be responsive to medical therapy and those patients in whom constriction will reverse or resolve (11, 12, 13).
Effusive-constrictive pericarditis
Effusive-constrictive pericarditis is the term for residual constrictive physiology after drainage of a pericardial effusion, usually due to pericardial inflammation (4). Echocardiography and cardiac MRI are used to evaluate the physiology and degree of inflammation.
Diagnosis references
1. Adler Y, Charron P, Imazio M, et al: 2015 ESC Guidelines for the diagnosis and management of pericardial diseases: The Task Force for the Diagnosis and Management of Pericardial Diseases of the European Society of Cardiology (ESC). Endorsed by: The European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2015;36(42):2921–2964. doi:10.1093/eurheartj/ehv318
2. Cremer PC, Klein AL, Imazio M. Diagnosis, Risk Stratification, and Treatment of Pericarditis: A Review. JAMA. 2024;332(13):1090-1100. doi:10.1001/jama.2024.12935
3. Schulz-Menger J, Collini V, Gröschel J, et al. 2025 ESC Guidelines for the management of myocarditis and pericarditis. Eur Heart J. 2025;46(40):3952-4041. doi:10.1093/eurheartj/ehaf192
4. Wang TKM, Klein AL, Cremer PC, et al. 2025 Concise Clinical Guidance: An ACC Expert Consensus Statement on the Diagnosis and Management of Pericarditis: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2025;86(25):2691-2719. doi:10.1016/j.jacc.2025.05.023
5. Antonopoulos AS, Vrettos A, Androulakis E, et al. Cardiac magnetic resonance imaging of pericardial diseases: a comprehensive guide [published correction appears in Eur Heart J Cardiovasc Imaging. 2024 Feb 22;25(3):e104]. Eur Heart J Cardiovasc Imaging. 2023;24(8):983-998. doi:10.1093/ehjci/jead092
6. Mathur AP, Saini A, Lucas BP, AlYousef T, Margeta B, Mba B: Diagnostic accuracy retrospectively of electrocardiographic findings and cancer history for tamponade in patients determined to have pericardial effusion by transthoracic echocardiogram. Am J Cardiol. 2013;111(7):1062–1066. doi:10.1016/j.amjcard.2012.11.064
7. Klein AL, Abbara S, Agler DA, et al: American Society of Echocardiography clinical recommendations for multimodality cardiovascular imaging of patients with pericardial disease: endorsed by the Society for Cardiovascular Magnetic Resonance and Society of Cardiovascular Computed Tomography. J Am Soc Echocardiogr. 2013;26(9):965–1012.e15. doi: 10.1016/j.echo.2013.06.023
8. Reuss CS, Wilansky SM, Lester SJ, et al. Using mitral 'annulus reversus' to diagnose constrictive pericarditis. Eur J Echocardiogr. 2009;10(3):372-375. doi:10.1093/ejechocard/jen258
9. Welch TD, Ling LH, Espinosa RE, et al. Echocardiographic diagnosis of constrictive pericarditis: Mayo Clinic criteria. Circ Cardiovasc Imaging. 2014;7(3):526-534. doi:10.1161/CIRCIMAGING.113.001613
10. Welch TD. Constrictive pericarditis: diagnosis, management and clinical outcomes. Heart. 2018;104(9):725-731. doi:10.1136/heartjnl-2017-311683
11. Cremer PC, Tariq MU, Karwa A, et al. Quantitative assessment of pericardial delayed hyperenhancement predicts clinical improvement in patients with constrictive pericarditis treated with anti-inflammatory therapy. Circ Cardiovasc Imaging. 2015;8(5):e003125. doi:10.1161/CIRCIMAGING.114.003125
12. Feng D, Glockner J, Kim K, et al. Cardiac magnetic resonance imaging pericardial late gadolinium enhancement and elevated inflammatory markers can predict the reversibility of constrictive pericarditis after antiinflammatory medical therapy: a pilot study. Circulation. 2011;124(17):1830-1837. doi:10.1161/CIRCULATIONAHA.111.026070
13. Miranda WR, Oh JK. Constrictive Pericarditis: A Practical Clinical Approach. Prog Cardiovasc Dis. 2017;59(4):369-379. doi:10.1016/j.pcad.2016.12.008
Treatment of Pericarditis
Nonsteroidal anti-inflammatory drugs (NSAIDs), and colchicineNonsteroidal anti-inflammatory drugs (NSAIDs), and colchicine
Sometimes systemic glucocorticoids or interleukin-1 inhibitors
Pericardiocentesis for tamponade and some large effusions
Sometimes intrapericardial medications (eg, triamcinolone)Sometimes intrapericardial medications (eg, triamcinolone)
Sometimes pericardial resection
Treatment of the cause (eg, cancer)
First-line therapy for uncomplicated pericarditis is aspirin (325 to 650 mg orally every 4 to 6 hours) or another NSAID (eg, ibuprofen 600 to 800 mg orally every 6 to 8 hours), usually in combination with colchicine (eg, 0.5 or 0.6 mg once or twice daily) (First-line therapy for uncomplicated pericarditis is aspirin (325 to 650 mg orally every 4 to 6 hours) or another NSAID (eg, ibuprofen 600 to 800 mg orally every 6 to 8 hours), usually in combination with colchicine (eg, 0.5 or 0.6 mg once or twice daily) (1, 2). A proton pump inhibitor should be considered to improve the gastric tolerability of NSAIDs. The intensity of therapy is dictated by the patient’s distress. Severe pain may require opioids. Risk of recurrence may be decreased with NSAID treatment if the duration of treatment is 3 to 4 weeks, but this approach has not been studied adequately. Colchicine for 3 months as an adjunct significantly decreases the recurrence rate and symptom persistence in patients with a first episode of acute pericarditis and is often used as first-line therapy (). A proton pump inhibitor should be considered to improve the gastric tolerability of NSAIDs. The intensity of therapy is dictated by the patient’s distress. Severe pain may require opioids. Risk of recurrence may be decreased with NSAID treatment if the duration of treatment is 3 to 4 weeks, but this approach has not been studied adequately. Colchicine for 3 months as an adjunct significantly decreases the recurrence rate and symptom persistence in patients with a first episode of acute pericarditis and is often used as first-line therapy (3). Glucocorticoids may be used if NSAIDs are contraindicated (1).
Strenuous exercise, including competitive sports, should be restricted (ideally limiting heart rate to < 100 beats per minute) for at least one month and maintained until symptoms, inflammation, and electrocardiographic changes resolve (2, 4). The goal is to limit the heart rate and reduce pain and inflammation caused by pericardial friction (1). Beta blockade or ivabradine may also be useful for this purpose. A graduated return to exercise should be employed. ). Beta blockade or ivabradine may also be useful for this purpose. A graduated return to exercise should be employed.
Although most mild cases of idiopathic and viral pericarditis respond well within a week, the optimal duration of treatment is unclear. Typically, patients should be treated at least until any effusion and evidence of inflammation (eg, elevated erythrocyte sedimentation rate or C-reactive protein levels) have resolved.
Hospitalization is warranted for some patients with an initial episode of acute pericarditis, particularly those with moderate or large effusions or with high-risk features, such as elevated temperature, subacute onset, immunosuppression, recent trauma, oral anticoagulant therapy, failure to respond to an initial course of aspirin or NSAIDs, and myopericarditis. Hospitalization is needed to determine etiology and to observe for the development of cardiac tamponade. Close, early follow-up is important in patients who are not hospitalized. Possible causative medications (eg, anticoagulants, procainamide, phenytoin) are stopped. For cardiac tamponade, immediate pericardiocentesis (see figure Hospitalization is warranted for some patients with an initial episode of acute pericarditis, particularly those with moderate or large effusions or with high-risk features, such as elevated temperature, subacute onset, immunosuppression, recent trauma, oral anticoagulant therapy, failure to respond to an initial course of aspirin or NSAIDs, and myopericarditis. Hospitalization is needed to determine etiology and to observe for the development of cardiac tamponade. Close, early follow-up is important in patients who are not hospitalized. Possible causative medications (eg, anticoagulants, procainamide, phenytoin) are stopped. For cardiac tamponade, immediate pericardiocentesis (see figure) is performed; removal of even a small volume of fluid may be lifesaving.

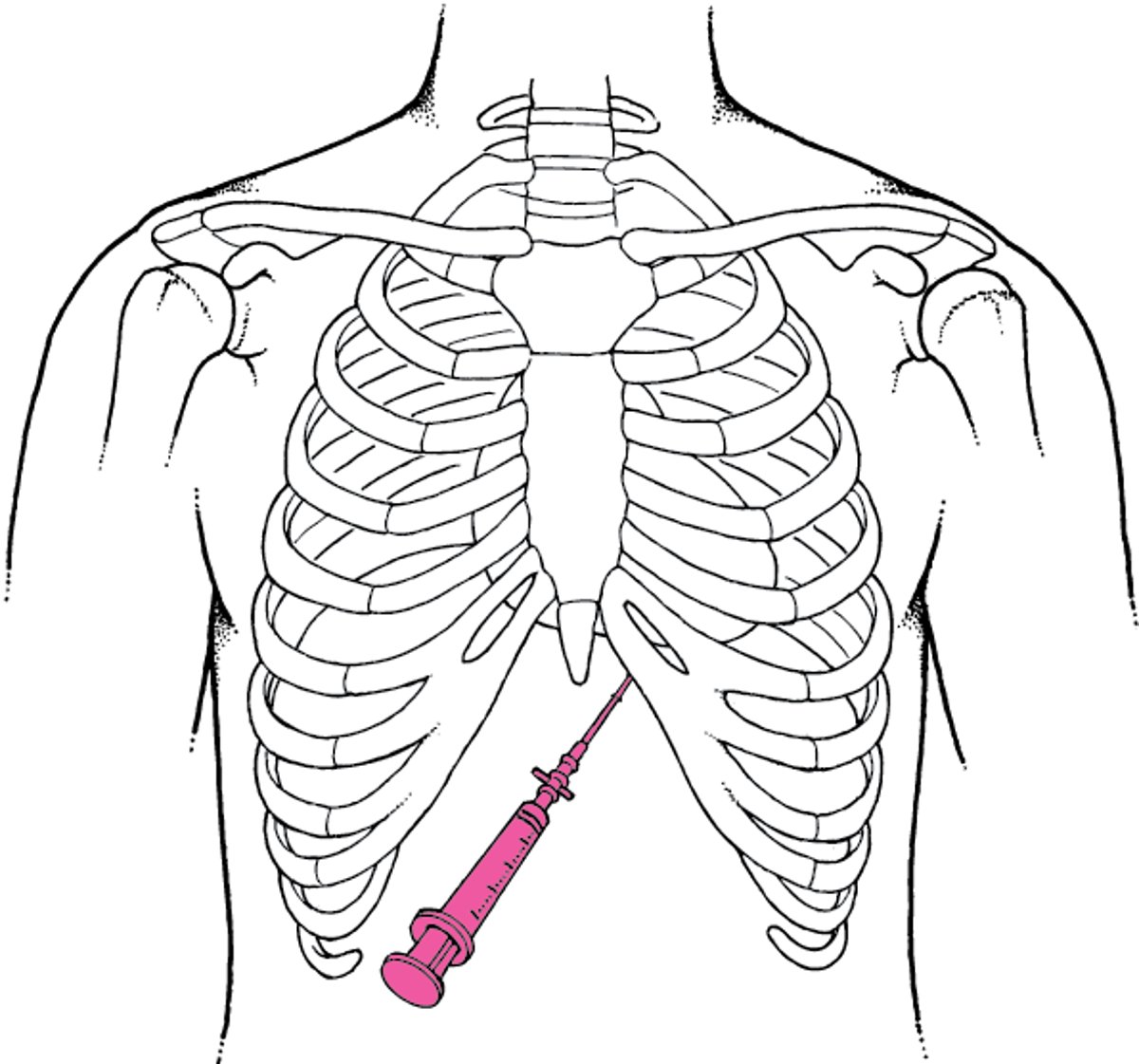
Pericardiocentesis
Except in emergencies (eg, cardiac tamponade), pericardiocentesis, a potentially lethal procedure, should be performed using echocardiographic guidance in a cardiac catheterization laboratory and should be supervised by a cardiologist or thoracic surgeon if possible. Resuscitation equipment must be at hand. IV sedation (eg, morphine 0.1 mg/kg or fentanyl 25 to 50 microgram plus midazolam 3 to 5 mg) is desirable. The patient should be recumbent, with the head elevated 30Except in emergencies (eg, cardiac tamponade), pericardiocentesis, a potentially lethal procedure, should be performed using echocardiographic guidance in a cardiac catheterization laboratory and should be supervised by a cardiologist or thoracic surgeon if possible. Resuscitation equipment must be at hand. IV sedation (eg, morphine 0.1 mg/kg or fentanyl 25 to 50 microgram plus midazolam 3 to 5 mg) is desirable. The patient should be recumbent, with the head elevated 30° from the horizontal. Under aseptic conditions, the skin and subcutaneous tissues are infiltrated with lidocaine. Under aseptic conditions, the skin and subcutaneous tissues are infiltrated with lidocaine. A 75-mm short-beveled, 16-gauge needle is attached via a 3-way stopcock to a 30- or 50-mL syringe. The pericardium may be entered via the right or left xiphocostal angle or from the tip of the xiphoid process with the needle directed inward, upward, and close to the chest wall. The needle is advanced with constant suction applied to the syringe. Echocardiography may be used to guide the needle as agitated saline is injected through it. Echocardiography can also be used to identify the optimal puncture site and the needle trajectory. Once in place, the needle should be clamped next to the skin to prevent it from entering further than necessary and possibly puncturing the heart or injuring a coronary vessel. ECG monitoring is essential for detecting arrhythmias produced when the myocardium is touched or punctured. As a rule, right atrial pressure and pulmonary artery occlusion pressure (pulmonary capillary wedge pressure) are monitored. Fluid is withdrawn until intrapericardial pressure falls below right atrial pressure, usually to subatmospheric levels. If continued drainage is needed, a plastic catheter may be passed through the needle into the pericardium and the needle withdrawn. The catheter may be removed when drainage is less than 25–50 mL/24 hours (usually 2–4 days). |

For patients who do not respond to therapy with NSAIDs and colchicine, determination of the specific phenotype guides further treatment. For patients with an "inflammatory phenotype," with fever, elevated C-reactive protein (CRP), and/or inflammation seen on cardiac MRI, interleukin-1 (IL-1) inhibitors (eg, anakinra, rilonacept, goflikicept) are preferred as second-line therapy (For patients who do not respond to therapy with NSAIDs and colchicine, determination of the specific phenotype guides further treatment. For patients with an "inflammatory phenotype," with fever, elevated C-reactive protein (CRP), and/or inflammation seen on cardiac MRI, interleukin-1 (IL-1) inhibitors (eg, anakinra, rilonacept, goflikicept) are preferred as second-line therapy (2). For the "non-inflammatory phenotype" (eg, low or near-normal CRP), glucocorticoids at low to moderate doses (eg, prednisone 0.2 to 0.5 mg/kg/day) remains standard therapy. An IL-1 inhibitor may also be used to reduce glucocorticoid use in patients who are steroid dependent (). For the "non-inflammatory phenotype" (eg, low or near-normal CRP), glucocorticoids at low to moderate doses (eg, prednisone 0.2 to 0.5 mg/kg/day) remains standard therapy. An IL-1 inhibitor may also be used to reduce glucocorticoid use in patients who are steroid dependent (1). Tuberculous and pyogenic pericarditis should be excluded before glucocorticoid therapy is initiated.
High-dose glucocorticoids (eg, prednisone 60 to 80 mg orally once a day) may initially be used in patients when required for other indications (eg, systemic lupus erythematosus, autoimmune or uremic pericarditis) but are not given routinely because they enhance viral multiplication and recurrence is common when the dosage is tapered; colchicine may be particularly useful during the glucocorticoid taper. An alternative approach that may have a lower rate of recurrence is the use of prednisone at a lower dose for 2 to 4 weeks followed by a slow taper over approximately 3 months. Intrapericardial instillation of triamcinolone 300 mg/mHigh-dose glucocorticoids (eg, prednisone 60 to 80 mg orally once a day) may initially be used in patients when required for other indications (eg, systemic lupus erythematosus, autoimmune or uremic pericarditis) but are not given routinely because they enhance viral multiplication and recurrence is common when the dosage is tapered; colchicine may be particularly useful during the glucocorticoid taper. An alternative approach that may have a lower rate of recurrence is the use of prednisone at a lower dose for 2 to 4 weeks followed by a slow taper over approximately 3 months. Intrapericardial instillation of triamcinolone 300 mg/m2 avoids systemic adverse effects and is highly effective but is typically reserved for patients with recurrent or refractory disease (1).
Current guidelines position anti-Interleukin-1 therapy (anakinra, rilonacept, goflikicept) as the key steroid-sparing option (second-line therapy after NSAID and colchicine) for recurrent inflammatory phenotype pericarditis, rather than glucocorticoids(Current guidelines position anti-Interleukin-1 therapy (anakinra, rilonacept, goflikicept) as the key steroid-sparing option (second-line therapy after NSAID and colchicine) for recurrent inflammatory phenotype pericarditis, rather than glucocorticoids(1).
The 2025 guidance supports an expanded role of cardiac MRI and to a lesser extent CT scans. Cardiac MRI documents inflammation, guides escalation and de-escalation, and aids in return to activity recommendations. CT remains important for pericardial thickness and calcification, and identification of constrictive physiology.
Anticoagulants are usually contraindicated in acute pericarditis because they may cause intrapericardial bleeding and even fatal tamponade; however, they can be given in early pericarditis complicating acute MI. Uncommonly (eg, with chronic constrictive pericarditis), pericardial resection is required.
Painful recurrences of acute pericarditis may respond to NSAIDs and/or twice daily colchicine for 6 to 12 months with a gradual taper. If these medications do not suffice, glucocorticoids or IL-1 inhibitors may be used [Painful recurrences of acute pericarditis may respond to NSAIDs and/or twice daily colchicine for 6 to 12 months with a gradual taper. If these medications do not suffice, glucocorticoids or IL-1 inhibitors may be used [5]); however, infection should be excluded first (1). Hydroxychloroquine is an option for recurrences refractory to glucocorticoids or IL-1 inhibitors.). Hydroxychloroquine is an option for recurrences refractory to glucocorticoids or IL-1 inhibitors.
Infections are treated with specific antimicrobials. Complete drainage is often necessary. For tuberculous pericarditis without coexistent HIV infection, glucocorticoids are an important adjunct to prevent constrictive disease (1).
In postpericardiotomy syndrome, post-MI syndrome, or idiopathic pericarditis, antibiotics are not indicated. Management is similar to that of acute pericarditis from other causes (1). But many months of treatment may be needed. Prophylactic colchicine may reduce the incidence of postpericardiotomy syndrome after cardiac surgery. ). But many months of treatment may be needed. Prophylactic colchicine may reduce the incidence of postpericardiotomy syndrome after cardiac surgery.Aspirin should be used when pericarditis occurs in patients with an acute myocardial infarction.
For pericardial effusion due to trauma, surgery is sometimes required to repair the injury and remove blood from the pericardium.
For pericarditis due to rheumatic fever, another systemic rheumatic disease, or tumor, therapy is directed at the underlying process.
Pericarditis due to uremia may respond to increased frequency of hemodialysis, aspiration, or systemic or intrapericardial glucocorticoids. Intrapericardial triamcinolone may be useful.Pericarditis due to uremia may respond to increased frequency of hemodialysis, aspiration, or systemic or intrapericardial glucocorticoids. Intrapericardial triamcinolone may be useful.
Chronic effusions are best treated by treating the cause, if known. Recurrent or persistent symptomatic effusions may be treated with balloon pericardiotomy or a surgical pericardial window (6). Asymptomatic effusions of unknown cause may require only observation.
Management of constrictive pericarditis
Measures that minimize the risk of developing constrictive pericarditis include the following (7):
Timely guideline-based treatment of acute and recurrent pericarditis
Complete drainage of infected pericardial effusions
In patients undergoing pericardiotomy, prophylactic colchicine and drainage of postpericardiotomy pericardial effusionsIn patients undergoing pericardiotomy, prophylactic colchicine and drainage of postpericardiotomy pericardial effusions
Patients with newly diagnosed constrictive pericarditis who are hemodynamically stable and without evidence of chronic constriction may be given a 3-month trial of anti-inflammatory medications, rather than pericardiectomy (2). Patients with pericardial inflammation on MRI may also benefit from a trial of pharmacotherapy first, rather than pericardiectomy.
Congestion in chronic constrictive pericarditis may be alleviated with salt restriction and diuretics. Digoxin is indicated only if atrial arrhythmias or ventricular systolic dysfunction is present. Congestion in chronic constrictive pericarditis may be alleviated with salt restriction and diuretics. Digoxin is indicated only if atrial arrhythmias or ventricular systolic dysfunction is present.
Patients with symptomatic constrictive pericarditis (eg, with dyspnea, unexplained weight gain, a new or increased pleural effusion, or ascites) and those with markers of chronic constriction (eg, cachexia, atrial fibrillation, hepatic dysfunction, pericardial calcification) usually require pericardial resection. Operative mortality from surgical pericardiectomy for constrictive pericarditis is approximately 5% (8). In addition, patients with mild symptoms (because they derive little benefit), heavy calcification, or extensive myocardial damage may be poor surgical candidates. Patients who have constrictive pericarditis due to irradiation or a systemic rheumatic disease are also more likely to have severe myocardial damage and may not benefit from pericardial resection.
Radical pericardiectomy may be performed for medically refractory pericarditis or chronic constrictive pericarditis; emphasis is placed on treating the cause of constrictive pericarditis, and referring complex cases specialized pericardial centers (1, 2).
Treatment references
1. Schulz-Menger J, Collini V, Groschel J, et al. 2025 ESC guidelines for the management of myopericarditis and pericarditis. Eur Heart J. 2025;46(40);3952-4041. doi:10.1093/eurheartj/ehaf192
2. Wang TKM, Klein AL, Cremer PC, et al. 2025 Concise Clinical Guidance: An ACC Expert Consensus Statement on the Diagnosis and Management of Pericarditis: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2025;86(25):2691-2719. doi:10.1016/j.jacc.2025.05.023
3. Imazio M, Brucato A, Cemin R, et al. A randomized trial of colchicine for acute pericarditis. N Engl J Med. 2013;369(16):1522–1528. doi:10.1056/NEJMoa1208536
4. Sivalokanathan S, Chokshi N. Pericarditis in Athletes: Approach to Exercise Restriction. Latest in Cardiology. September 7, 2022. Accessed January 15, 2026.
5. Abadie BQ, Cremer PC. Interleukin-1 Antagonists for the Treatment of Recurrent Pericarditis. BioDrugs. 2022;36(4):459–472. doi:10.1007/s40259-022-00537-7
6. Hoit BD. Pericardial Effusion and Cardiac Tamponade Pathophysiology and New Approaches to Treatment. Curr Cardiol Rep. 2023;25(9):1003–1014. doi:10.1007/s11886-023-01920-8
7. Lazaros G, Vlachopoulos C, Lazarou E, Tsioufis K. New Approaches to Management of Pericardial Effusions. Curr Cardiol Rep. 2021;23(8):106. doi:10.1007/s11886-021-01539-7
8. Al-Kazaz M, Klein AL, Oh JK, et al. Pericardial Diseases and Best Practices for Pericardiectomy: JACC State-of-the-Art Review. J Am Coll Cardiol. 2024;84(6):561-580. doi:10.1016/j.jacc.2024.05.048
Key Points
Patients with pericarditis have symptoms signs, and diagnostic findings suggestive of pericardial inflammation and/or fluid accumulation (effusion).
Blood tests, electrocardiography, echocardiography, and cardiac MRI are used for diagnosis, but right and left heart catheterization or CT may also may be needed to diagnose constrictive pericarditis.
Inflammation is treated with nonsteroidal anti-inflammatory drugs and/or colchicine and temporary exercise restriction; interleukin-1 inhibitors or glucocorticoids may be added for selected patients in whom the cause is noninfectious.Inflammation is treated with nonsteroidal anti-inflammatory drugs and/or colchicine and temporary exercise restriction; interleukin-1 inhibitors or glucocorticoids may be added for selected patients in whom the cause is noninfectious.
Effusions usually respond to treatment of the cause, but recurrent or persistently symptomatic effusions may require drainage (percutaneous or surgical).
Symptomatic chronic constrictive pericarditis usually requires pericardial resection, although patients with early stage constrictive pericarditis can be treated with a trial of pharmacotherapy first.
Drug Information for the Topic





